{kind=link}

Date: Thu, 20 Mar 2003 19:35:29 EST
Subject: Popliteal injuries and tibial plateau fractures
I was consulted on a 40 year old man who fell or jumped from a three story building and sustained an axial loading tibial plateau fracture with anterior displacement of the distal fragment.
Pulses were absent until reduction when they returned.
I was asked to do an arteriogram of the popliteal artery.
How does the group feel about angiography for tibial plateau fractures caused by blunt trauma that result in transient pulse deficit that resolves with reduction? When would you do it?
Sal Sclafani, MD
SUNY Downstate
From: ecthompson
Date: Thu, 20 Mar 2003 20:46:15 -0600
I'm not sure that anything else needs to be done. From Eric's work and my small series, a normal pulse equals no need for operative intervention. Now, if the pulse isn't normal, a-gram.
Errington C. Thompson, MD
Trauma Surgeon
Trinity Mother Frances
Tyler, Tx
From: SJASMD
Date: Thu, 20 Mar 2003 23:19:39 EST
who said anything about operative therapy? Let's deal with the diagnosis first.
I was asking about the indications for an arteriogram in tibial plateau fractures. I have never consider these to be the same as knee dislocations.
What if the pulse was absent on admission and then returned after reduction. Does that impact on your decision process?
What if the pulse is absent and remains absent with a tibial plateau fracture?
sal
Date: Fri, 21 Mar 2003 00:44:23 -0500
From: Bill Burman
Sal
High energy tibial plateau fractures have a significant incidence of vascular injury. See Mark Reilly's OTA BFC Lecture:
He says:
"It is critical to recognize that a Schatzker type IV fracture frequently represents a reduced fracture dislocation of the knee, and the neurologic and vascular concerns which accompany knee dislocations apply to these fractures as well."
High energy proximal tibia fractures are at risk for trifurcation injury.
The question of whether a fracture/dislocated limb which had no pulses but then had return of pulses following limb realignment/reduction needs angio does not seem to have been addressed by a recent rather extensive OTA-AAST discussion on this subject.
The EAST peripheral vascular injury algorithm does not include a break point for limb realignment/reduction and therefore is not as specific as Jack Wilber's OTA BFC peripheral vascular injury algorithm which suggests clinical observation if normal pulses (in the absence of any other hard signs of vascular injury) return.
From: SJASMD
Date: Fri, 21 Mar 2003 04:08:53 EST
Bill
Great review and good call on the fracture type.
I have noted few popliteal injuries associated with tibial plateau fractures.. Absent pulses are not infreuent prior to reduction and I have not been interested in performing arteriogaphy in such situations.
In this case I deferred to my surgical colleague, an excellent trauma surgeon who wanted to put this patient to bed with knowledge of any potential injury.
The arteriogram is shown here:
|
This shows four areas of filling defects consistent with intimal tears throughout the popliteal artery. The flaps moved with flow, looking like a valve. The flaps were proximally based.
what are the treatment options?
Sal
From: ecthompson
Date: Fri, 21 Mar 2003 05:38:16 -0600
Why would Tibial plateau fractures be any different?
If I have a normal pulse, then my diagnosis is normal vessel. If there pulse is diminished then an a-gram is indicated. If there is a question then ABI's can be performed.
Errington C. Thompson, MD
Trauma Surgeon
Trinity Mother Frances
Tyler, Tx
From: Frykberg, Eric
Date: Fri, 21 Mar 2003 06:53:29 -0500
How does the group feel about angiography for tibial plateau fractures caused by blunt trauma that result in transient pulse deficit that resolves with reduction? When would you do it?
There is no need for this--the absence of any hard signs (NOT just pulse) excludes a vascular injury as well as angio or any other diagnostic modality, and more cheaply--of course you only mentioned the pulse, but I assume there are no other hard signs either. Pulse status alone is not reliableenough to make this decision. The evidence in the literature on this--not only trauma and vascular, but also orthopedic--is quite clear on this-- and there is NO published evidence to support angio in this circumstance. Certainly if there is some doubt about whether a pulse is present, or about the presence of any other hard sign, then certainly an angio is indicated.
Let's be clear here, E, and others--pulse alone is not enough--we must remember that the 5 hard signs as a group must be assessed for the proper decision to be made. When NO hard sign is present, a vascular injury requiring surgical repair has been ruled out as accurately as with any other modality. Pulse is just one of 5 hard signs, and by itself cannot do this--a major vascular injury can still be present in the presence of a pulse. so any presentation or answer here must depend on the status of all 5 hard signs.
Sal-- As was predictable, you did not need the arteriogram as predicted by the absence of hard signs. The injury you found is nonocclusive, of a type that may be found in about 10% of cases in the absence of hard signs, and needs no surgical Rx--as has been shown by an accumulation of 14 years of trauma, interventional radiologic and vascular literature from several centers, and without any data to refute it. You would have a hard time justifying any surgical attack on this. Certainly the limb must be monitored for any development of hard signs, and having gotten this angio (which I would not have), I would do a followup in about a week--at which time we know there is about a 90% chance it will have spontaneously resolved. Any development of hard signs, or any angiographic deterioration (extravasation or occlusion) requires surgery at that time--in which case there is no morbidity ever once yet recorded from the delay. any one may disagree with this, but like my assertion, such disagreement means nothing in the absence of supporting data that refutes the existing trove of data to the contrary.
Date: Fri, 21 Mar 2003 11:40:06 -0800
From: Bruce Sangeorzan
in our series, patients with ABI> .95 did not have positive arteriography or treatable vascular injuries.
From: SJASMD
SJASMD: How does the group feel about angiography for tibial plateau fractures caused by blunt trauma that result in transient pulse deficit that resolves with reduction? When would you do it?
Fri, 21 Mar 2003 06:53:29 -0500 Frykberg, Eric wrote: There is no need for this--the absence of any hard signs (NOT just pulse) excludes a vascular injury
Eric, the absence of hard signs did not exclude a vascular injury as is shown by the injury on this arteriogam. Perhaps not a operative lesion but surely we have an injury here.
Fri, 21 Mar 2003 06:53:29 -0500 Frykberg, Eric wrote: Sal-- The injury you found is nonocclusive, of a type that may be found in about 10% of cases in the absence of hard signs, and needs no surgical Rx--.............. You would have a hard time justifying any surgical attack on this.
Eric: we agree that this injury does not require surgical attack. There are nonsurgical options in my management of this injury, such platelet inhibition to decrease risks of emboli and occlusion . Followup imaging and heightened surveillance are valuable in our experience. The orientation of intimal flaps helps predict outcome. Gently tacking the flaps back into the defects with a compliant balloon decreases the time and area of exposure of the media and perhaps decreases the risk of occlusion. Certainly popliteal occlusion has higher morbidity than nonocclusive injury.
As you know, my interests in this subject are academic . My goal is to continue to assess the natural history of these lesions. My study of these lesions has been rigorous and my followup is very detailed. All arteriographic abnormalities are reimaged until they revert to normal appearance. I only regret that I have not been able to follow my patients for the time needed to assess the risks for arteriosclerosis at sites of injury.
In general my conclusions are the same as yours. Our differences are in general also "minimal". My experience with those minimal injuries is just not as satisfying or benign as yours.
Sal
From: SJASMD
Date: Sat, 22 Mar 2003 07:21:27 EST
Fri, 21 Mar 2003 11:40:06 -0800 Bruce Sangeorzan wrote: in our series, patients with ABI> .95 did not have positive arteriography or treatable vascular injuries.
I think it might be difficult to assess ABI in this injured extremity.We did not do it.
Perhaps it is my radiological point of view. I see the purpose of imaging to determine that there is an injury, not only to see if there is a surgically correctible injury.
Radiologists injure vessels every day with good intention. We know that balloon angioplasty for atherosclerosis creates an injury that is similar to injury caused by other methods of stretch such as this fracture dislocation. While we are comfortable with observation of high flow vessels such as the iliacs, femoral and popliteal artery angioplasty does have a real risk of post procedural occlusion. Thus we TREAT with antiplatelet medications and anticoagulation in some circumstances. We may be using drug eluting stents soon.
Granted, the trauma baseline vascular status is different from the vasculopathy with atherosclerosis. Perhaps these nonsurgical interventions are not necessary in the trauma patient.This is not a general recommendation to the readership, only a statement of my academic interests. I will continue to evaluate the use of antiplatelet agents for these injuries.
sal sclafani
From: SJASMD
Date: Sat, 22 Mar 2003 07:34:15 EST
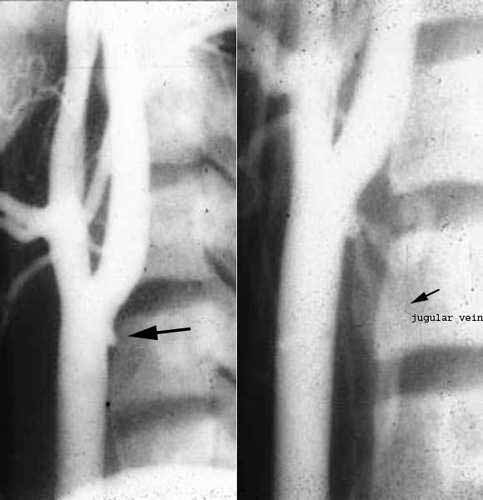
As Eric predicted, the appearance of this injury resolved and more quickly that expected. This followup arteriogram showed no evidence of the intimal injuries present four days earlier.
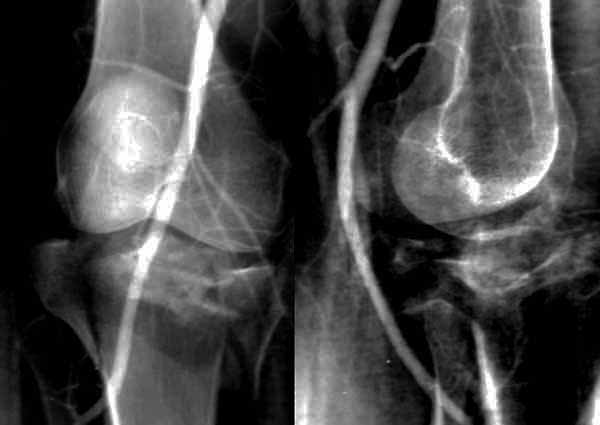 |
I conjecture that the orientation of the flaps which were proximally based lend themselves to readherence to the exposed media.
It is when the flaps are based distally that blood flow tends to undermine and locally dissect the wall of the vessel. Surely distally based flaps can also heal but they are more likely to persist or extend.
Whether the aspirin that was administered had any effect on the rapidity of this healing process is unproven.
sal sclafani
From: Frykberg, Eric
Date: Sat, 22 Mar 2003 08:42:28 -0500
Sal-- You were right in your correction of my response--I was not precise. The absence of hard signs reliably excludes SURGICALLY SIGNIFICANT vascular injuries, with an accuracy equivalent to any other diagnostic modality--in about 10% of cases, clinically occult vascular injuries will occur, with a benign natural history that is consistent enough that it does does not warrant even trying to find them--thus our practice recommendation that the absence of hard sings in THIS setting does not require A-gram , noninvasives etc--they do not need to be found. I agree that we do not differ in our essential approaches to these injuries. Also--your statement that YOUR experiences with these injuries are not as good as MINE is a bit inaccurate-accuracy dictates that you state that your experiences are not as good as anyone else who has published on this topic in the last decade, in addition to us--every other study of this issue from several other centers in addition to ours has demonstrated the same natural history, and the same lack of a single instance of limb morbidity whatsoever when the proper criteria are followed for using phys exam alone to make the clinical decisions in simple penetrating or blunt extremity trauma. Remember--your experience includes lesions--occlusive and extravasating lesions--which we do not watch, according to your 1997 paper. Of course watching such dangerous lesions will adversely skew your results. You need to compare apples to apples before you generalize. Your own paper showed the benign natural history of nonocclusive AND asymptomatic lesions that we did.
Thanks for this nice followup--a couple of points. We know that aspirin and antiplatelet or anticoagulation therapy is NOT necessary for this outcome--in all of our series we never once used them, as is true of several other published series, and these results--with hundreds of lesions and a 5-10 year F/U (J of Trauma, Feb 1998)-- are as good as any published--so the statement that their efficacy is unknown is not really accurate--their lack of efficacy is, in fact, known. Also--your statments indicating that orientation of the flap has any correlation whatever with outcome are completely unfounded. This is a good example of conjecture as to what sounds right being muddled with reality. There are no studies at all showing this to be true--only occasional conjecture like yours--and there IS hard evidence showing this NOT to be true--J of Trauma Feb 1998, J of Trauma May 1989, J of Trauma Aug 1989, J Vasc Surg Jan 1990, J of Trauma April 1991--note actual angio images in these papers of distal, upward-directed and large (>75% of lumen involved) flaps all of which have resolved no differently than any other form of flap. As long as the lesion is nonocclusive and asymptomatic (i.e. no hard signs), they all seem to behave equally benignly. If you have data to the contrary--again, using the same criteria--please let me know, as I've missed it.
 |
ERF
From: SJASMD
Date: Sat, 22 Mar 2003 13:33:30 EST
Rick
Our report Hoffer, et al, Natural History of Arterial Injuries Diagnosed with Arteriography JVIR 1997; 8:43-53 did discuss minimal injuries IN ADDITION TO more serious injuries. Of 23 intimal defects with arteriographic followup (avg 23.5d range 1-1900 days) , 11 normalized, two stenosed, three dilated (pseudoaneurysms), one persisted, two occluded, three developed false aneurysms, 1 developed an arteriovenous fistula. Those are our facts. Why they are different than other reports is more conjecture. Did all require therapy ultimately? No.
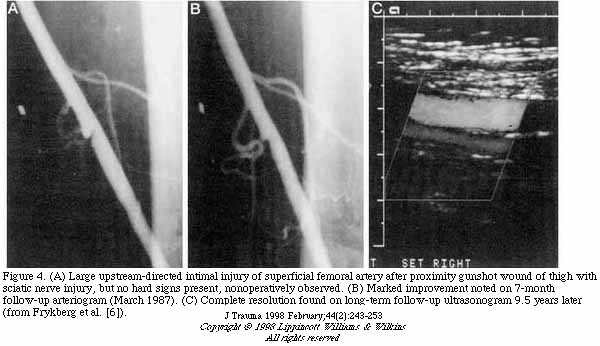
Here is an example of an asymptomatic minimal injury (a mural hematoma, not intimal flap) that did require operative therapy.
 |
This young man in his 20's sustained a shotgun wound to the thigh. Arteriography shows a mural hematoma. The five Ps were intact. He returned almost one year later, with a healed shotgun wound with a nonhealing heel ulcer resulting from the stricture of the SFA at the site of the intramural hematoma. Bypass was performed. Ulcer healed.
In a message dated 3/22/2003 11:06:14 AM Eastern Standard Time, eric.frykberg writes: We know that aspirin and antiplatelet or anticoagulation therapy is NOT necessary for this outcome--in all of our series we never once used them, as is true of several other published series, and these results--with hundreds of lesions and a 5-10 year F/U (J of Trauma, Feb 1998)-- are as good as any published--so the statement that their efficacy is unknown is not really accurate--their lack of efficacy is, in fact, known. If you have data to the contrary--again, using the same criteria--please let me know, as I've missed it.
I am not so sure. Certainly in critical vascular beds like the internal carotid artery we know emboli are secondary manifestations of intimal flaps. There are a number of reports in the literature regarding that.
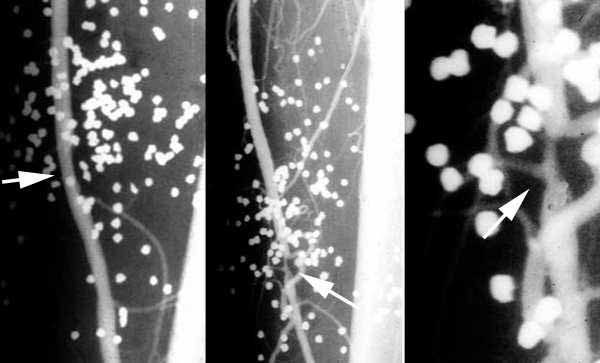
Here is a minimal injury not treated with antiplatelet therapy or anticoagulation. Perhaps the stroke on the fifth day, that led to the followup arteriogram that showed a arteriovenous fistula, might have been avoided.
 |
I guess we can avoid aspirin and accept emboli to the extremities since these injuries likely to remain asymptomatic. Since I have seen two intimal flaps result in occlusion, I shall continue to risk the aspirin.
In a message dated 3/22/2003 11:06:14 AM Eastern Standard Time, eric.frykbergwrites: Also--your statments indicating that orientation of the flap has any correlation whatever with outcome are completely unfounded. This is a good example of conjecture as to what sounds right being muddled with reality. There are no studies at all showing this to be true--only occasional conjecture like yours--and there IS hard evidence showing this NOT to be true--J of Truama Feb 1998, J of Trauma May 1989, J of Trauma Aug 1989, J Vasc Surg Jan 1990, J of Trauma April 1991--note actual angio images in these papers of distal, upward-directed and large (>75% of lumen involved) flaps all of which have resolved no differently than any other form of flap. As long as the lesion is nonocclusive and asymptomatic (i.e. no hard signs), they all seem to behave equally benignly. If you have data to the contrary--again, using the same criteria--please let me know, as I've missed it.
Sometimes conjecture is necessary because there are no clear answers.
 |
This asymptomatic patient with a gunshot wound of the knee had arteriography which showed a bulge and an intimal flap. A followup several days later showed expansion of either a pseudoaneurysm or a false aneurysm. The distally based flap is more prominent. We treated this with a stent graft. One year ultrasound followup showed patency of the stent graft.
Would this injury have healed spontaneously? I don't know. I would conjecture that it would not. Why did this asymptomatic patient expand the bulge? Was it the distally based flap, or was it the underlying pathology of the wall? Conjecture.
Sal
From: DocRickFry
Date: Sat, 22 Mar 2003 17:18:10 EST
In a message dated 3/22/2003 2:18:50 PM Eastern Standard Time, SJASMD writes: This young man in his 20s sustained a shotgun wound to the thigh. Arteriography shows a mural hematoma. The five Ps were intact. He returned almost one year later, with a healed shotgun wound with a nonhealing heel ulcer resulting from the stricture of the SFA at the site of the intramural hematoma. Bypass was performed. Ulcer healed.
Sal, you confirm our longstanding results here! That minority of cases that will develop problems will declare themselves by the development of symptoms--at which time an Agram should be done and the problem surgically repaired--and as you comfirm, no harm to the patient as a result of that delay not ONCE yet recorded! Much better to intervene on that small minority (<1% of all asymptomatic comers with proximity penetrating wounds like this) that will deteriorate than than operate unnecessarily on the other 99% routinely UNnecessarily! Also--that 0.8% miss rate using phys exam alone is the SAME 0.8% or so that would be missed by angio according to the well referenced literature in all studies of this issue, regardless of how much you my disagree with those reports (remember, your 1986 paper is one of those reports!)
Secondly--our published criteria DO state clearly that we would angio asymptomatic shotgun wounds in proximity to major vessels--again--you keep straying from apples over to oranges, again! But even in the case your present, it is not at all certain this injury would have been picked up on the initial go-round.
In a message dated 3/22/2003 3:44:08 PM Eastern Standard Time, SJASMD writes: Sometimes conjecture is necessary because there are no clear answers. This asymptomatic patient with a gunshot wound of the knee had arteriography which showed a bulge and an intimal flap. A followup several days later showed expansion of either a pseudoaneurysm or a false aneurysm. The distally based flap is more prominent. We treated this with a stent graft. One year ultrasound followup showed patency of the stent graft.
Again, Sal, I do not disagree--we KNOW that a tiny percentage of all comers will deteriorate in just this way--and when they do, they will develop hard signs enabling their detection and repair. The literature from us and others is quite clear--so you once again confirm my point. And--as here, and as our results again would have predicted, you fixed it when it happened, and the patient DID FINE--once again, not one single instance of limb morbidity ever yet reported as a result of nonop management of nonocclusive injuries. You have just added to those results!
Conjecture is sometimes necessary WHEN THERE ARE NO DATA one way or another--but NOT when the data is abundant and clear as in this issue. You are being a bit disingenuous in trying to make a point (actually, you are making MY point) with single anecdotal cases, too--things always look their worse if you pull up the worst single exceptions to the rule--and let's be clear, these are all exceptions, NOT the rule. In fact, these exceptions are well reported to occur--less than 1% of the time if phys exam alone is used to make your decisions on all limb trauma--but this is the same rate as they occur were angio, noninvasives, etc used as well! NO modality is 100% perfect, and all have the SAME very low miss rate ( Surg Clinics North Amer April 1995, Feb 1998 J of Trauma, JACS October 1996)--so in that case, outcomes all being equal, of course the modality of choice hinges on the least expensive, safest, and most widely applicable modality--in this case, the choice is clear
And, with that , I have once again--and with your help for confirmation-- summarized the abundant body of published work on this topic over the past 14 years, which has yet to be refuted in a single report. A few ATTEMPTS to refute--but nonetheless unrefuted still. Sounds like it may actually be correct, no?
ERF
From: SJASMD
Date: Sat, 22 Mar 2003 22:23:31 EST
In a message dated 3/22/2003 5:22:14 PM Eastern Standard Time, DocRickFry writes: Sal, you confirm our longstanding results here! That minority of cases that will develop problems will declare themselves by the development of symptoms--at which time an Agram should be done and the problem surgically repaired--and as you comfirm, no harm to the patient as a result of that delay not ONCE yet recorded!
Since when is a heel ulcer no harm
In a message dated 3/22/2003 5:22:14 PM Eastern Standard Time, DocRickFry writes: But even in the case you present, it is not at all certain this injury would have been picked up on the initial go-round.
The injury WAS picked up on the initial go round.
In a message dated 3/22/2003 5:52:15 PM Eastern Standard Time, DocRickFry writes: Again, Sal, I do not disagree--we KNOW that a tiny percentage of all comers will deteriorate in just this way--and when they do, they will develop hard signs enabling their detection and repair. The literature from us and others is quite clear--so you once again confirm my point. And--as here, and as our results again would have predicted, you fixed it when it happened, and the patient DID FINE--once again, not one single instance of limb morbidity ever yet reported as a result of nonop management of nonocclusive injuries. You have just added to those results!
Rick
Stop the spin. The case is an illustration against your point that if there are no signs, there is no injury and that all benign lesions act benignly.
As long as the lesion is nonocclusive and asymptomatic (i.e. no hard signs), they all seem to behave equally benignly. If you have data to the contrary--again, using the same criteria--please let me know
This is not an absolute as you should state it that way. The purpose was not to show that the outcome would be unchanged by delayed diagnosis and treatment but that distally based flaps can deteriorate.
Let's move on.
Sal
From: DocRickFry
Date: Sat, 22 Mar 2003 23:09:13 EST
In a message dated 3/22/2003 10:24:46 PM Eastern Standard Time, SJASMD writes: Since when is a heel ulcer no harm
When it has healed and the case was a success, as you stated--did I miss something?
In a message dated 3/22/2003 10:35:53 PM Eastern Standard Time, SJASMD writes: Stop the spin. The case is an illustration against your point that if there are no signs, there is no injury and that all benign lesions act benignly.
Sal--
Why do you keep spinning this way? I have continued to state, here and in all our papers, that ALL do NOT resolve--some do deteriorate--do you not read what is written? I guess I am speaking a different language...
In a message dated 3/22/2003 10:35:53 PM Eastern Standard Time, SJASMD writes: This is not an absolute as you should state it that way. The purpose was not to show that the outcome would be unchanged by delayed diagnosis and treatment but that distally based flaps can deteriorate. Let's move on.
Once again--who are you arguing with? This was a given from the beginning--read our papers once again--apparently you've forgotten--we have been stating this--we are the ones that demonstrated just this as far back as 1988.. This was not the issue--the issue is, the proper perspective is, just as it is with angio thatt the number of misses, and the number that do deteriorate, is a small fraction of the total. Thus, you cannot argue to treat the majority for what happens to a small minority--glad you finally agree...
We could all post cases of angiograp\hic misses as well--and state " I just wanted to be clear that there are missed injuries with angio"--well, no kidding! Who argues that? You yourself have shown that. But, so what? Does that mean angio is no good as a diagnostic modality? Of course not! Why? Because it is not true in the great majority of cases--just a matter of understanding the limits of any approach.
ERF
From: fvmclbooth
Date: Sun, 23 Mar 2003 02:03:46 -0500
Rick
Whilst it's probably not sufficient evidence to derail the minimalist intervention approach you espouse, I believe Sal described a patient who developed a non-healing ulcer of his foot following a delayed development of a stenosis. This in turn responded to a bypass. In the end we can agree that this turned out fine but I doubt very much if the owner of the ulcerated foot would subscribe to the statement "not one single instance of limb morbidity ever yet reported as a result of nonop management of nonocclusive injuries"
Moderation in all things, even firmly held opinions!
Frank Booth
From: DocRickFry
Date: Sun, 23 Mar 2003 06:43:16 EST
In a message dated 3/23/2003 2:07:19 AM Eastern Standard Time, fvmclbooth writes: but I doubt very much if the owner of the ulcerated foot would subscribe to the statement.. "not one single instance of limb morbidity ever yet reported as a result of nonop management of nonocclusive injuries". Moderation in all things, even firmly held opinions!
Frank--
Right you are!
ERF
From: SJASMD
Date: Sun, 23 Mar 2003 15:15:43 EST
I used this case as a way of discussing progression of intimal flaps.
I was surprised that there was no hue and cry about the use of a stent graft in the popliteal artery.
Any thoughts out there about the pros and cons of stent grafts of the popliteal artery?......
To reinterate:
This asymptomatic patient with a gunshot wound of the knee had arteriography which showd a bulge and an intimal flap. A followup several days later showed expansion of either a pseudoaneurysm or a false aneurysm. The distally based flap is more prominent. We treated this with a stent graft. One year ultrasound followup showed patency of the stent graft.
|
sal sclafani
From: DocRickFry
Date: Sun, 23 Mar 2003 20:49:30 EST
Any thoughts our there about the pros and cons of stent grafts of the popliteal artery?......
Sal--
I'll weigh in--I think it was a good idea worth trying. We need to gain an experience with the application of this technology to vascular lesions that we all agree require repair. Given the sparse experience overall, most especially in the politeal artery, these investigations are necessary--it would be of value to avoid surgery here if possible with equivalent outcome. Obviously this requires that such interventions be studied, and followed very carefully to report the outcomes--good or bad.
ERF
From: SJASMD
Date: Sun, 23 Mar 2003 22:28:03 EST
Followup will always be difficult with these injuries: I had compliance for a year but I have not been able to get this man back for further followup.
I have tried in three cases, two penetrating with success and one failure in a pop occlusion related to a knee dislocation. I could not get the wire to cross the popliteal artery.
The biggest reservation I have about stent grafting the knee has to do with repetitive motion of the joint with its effects on the intergrity of the stent and the degree of intimal hyperplasia related to the motion.
I have been interested now for a while in assessing the actual location of the bending of the artery with respect to bending of the knee. It appears that the vessel does not bend any where near the joint but actually higher near the adductor canal. Any thoughts on this?
Sal
From: DocRickFry
Date: Mon, 24 Mar 2003 12:25:25 EST
This is an interesting line of thought--your observation actually speaks in favor of a good outcome with stenting of the popliteal artery. One thing I have found over the years, probably like you, is how resilient and resistant to injury our vessels are overall.
ERF
From: SJASMD
Date: Mon, 24 Mar 2003 15:32:31 EST
One thing I have found over the years, probably like you, is how resilient and resistant to injury our vessels are overall.
unless the patient has a cardiac cath
Date: Mon, 24 Mar 2003 20:18:26 +0100
From: rikal
Hello, what is your procedure for on table-angio? Thank you.
Riccardo
From: SJASMD
Date: Mon, 24 Mar 2003 15:28:43 EST
what is your procedure for on table-angio?
For lower extremity:
sal Sclafani