Date: Sun, 10 Mar 2002 14:01:36 +0530
Subject: Polytrauma - limb salvage or ablation
Presenting this case for opinion of the list and discussion.
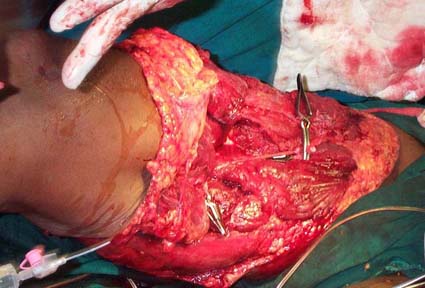
45 year old healthy male referred to our centre following a road accident. Arrived 3 hours after the injury. On arrival-patient in shock, bilateral haemopneumothorax, dislocation right elbow, lacerated large wound anteromedial,medial and postero medial aspect of right thigh dividing large bulk of muscles, femoral artery and femoral vein. Shaft of femur though exposed medially not fractured. Patient resuscitated immediately, bilateral intercostal drainage done, started on positive pressure ventillation, femoral vesels ligated to arrest bleeding, multiple blood transfusions given and then explored in operation theatre.
At exploration (less than 5 hours from the time of injury) sciatic nerve in continuity, retrograde bleeding from distal part of femoral artery and vein, calf not tense. Patient haemodynamically stable under general anaethesia. Urine output adequate.
|
My question to the list: Should we try to reconstruct vessels and preserve the limb in view of the following factors?
i) exploration within five hours of injury.
ii) sciatic nerve incontinuity?
iii) patient though arrived in shock could be resuscitated and parameters maintained under anaesthesia?
Or should we proceed to amputation and subsequent measures?
Obviously we cannot wait for the list discussion to take a decision. I will present what we have done and the follow up after the discussion.
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.
Date: Sun, 10 Mar 2002 9:15 am
From: Bill Burman
Key information appears to be missing here. What is the neuro exam distal to the vascular injury?
If this is rated as a "high energy" injury using a MESS score calculation (Click here for MESS Calculator) , the MESS Score would be:
MESS Score > 7 - poor limb viability prognosis
Date: Mon, 11 Mar 2002 00:52:13 +0530
From: DR T I GEORGE
We had a practical problem. The patient arrived in shock and had to go on ventillator immediately. Hence could not objectively assess distal neurological status. The intact sciatic nerve was our guide.
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.
Date: Sun, 10 Mar 2002 3:29 pm
From: Bill Burman
What about direct electrostimulation of the intact sciatic nerve and distal musculature? If no response, what about direct electrostimulation of the intact sciatic nerve and distal musculature after 30 minutes of femoral artery intraluminal shunt perfusion?
Date: Sun, 10 Mar 2002 19:55:24 -0500
From: Ernest Block, MD
since you may need to go to the OR to do some sort of damage control or amputation, you have little to lose by inserting a piece of tubing in each end of the torn vessel (a la Feliciano), and adding a fasciotomy. If bleeding increases in the soft tissues, I would bail. Given the duration of shock and general neglect of injuries (>3 hours), more work would not be appropriate IMHO.
With the exception of the realm of vascular surgery, it is still life over limb ;-)
eb
Date: Sun, 10 Mar 2002 20:30:11 EST
From: DocRickFry
Bill--
There is absolutely no reason why, once this patient has been stabilized and in the O.R, the femoral artery should not have immediately been reperfused--can be done in 5 minutes with a shunt of plastic tubing after distal embolectomy and then regional and/or systemic heparinization. Then, the same can be done with the vein, then, an immediate fasciotomy to assure outflow due to risk of compartment syndrome. THEN--you have all the time in the world for examining all the tissues, assuring nerve intact, debriding devitalized tissues, washing away gross contamination, doing whatever needs doing to the elbow and further resuscitating the patient, etc. The way the question was asked, it did not appear this was done in this order, which happens to be well documented in virtually all studies of complex extremity trauma as the biggest mistake made leading to limb loss--delay in revascularization and averting compartment syndrome sooner rather than later. The recent studies showing limb salvage rates in this setting of >90% all document aggressive reperfusion and fasciotomy as the major contributors to these successful results Don't ask questions in a case like this until AFTER perfusion of the distal extremity is assured--THEN see what you are left with. Otherwise you have a self-fulfilling prophesy, as ongoing warm ischemia while you scratch your head for a few hours is the one certain killer of limbs--not nerve damage, or broken bones, or ugly soft tissue wounds--perfusion! The intact nerve and the appearance of the tissues indicate to me this limb should be totally salvageable.
Don't worry about formal repair of the vessels--just take 5 minutes to restore perfusion. Such a little step that could make such a big difference. The literature and available data of the past 15 years is very clear that perfusion should ALWAYS come before any other tissue repair--references on request. Start with the EAST Practice Management Guidelines--combined vascular/skeletal extremity trauma under Penetrating Extremity Trauma--at www.east.org. (Adobe Acobat PDF file)
ERF
Date: Sun, 10 Mar 2002 21:43:37 -0600
From: ECThompson
I guess the only thing that I would add is that the MESS is worth about what we paid for it. A high MESS can be deceiving.
If I stab my patient in the groin with a thin knife (because I'm unstable, of course) that only transects the femoral artery and it takes 4 hours to get the patient to the ER. Whats this patients MESS? There would be no distal pulses. Because of lack of blood flow for a prolonged period of time there will not be neurologic function either. Should this patient have a primary amputation? No. A simple transection can be repaired in 30-60 minutes.
Reperfuse then reassess. Talk to patient then make a decision.
BTW, Im not much for shunts. In the middle of the night the nurses can't find them. They arent something that I use all the time therefore, it will take me sometime to get the shunt in and working. Might be able to fix the problem in that length of time.
E
Errington C. Thompson, MD, FACS
Trauma Surgeon
Trinity Mother Frances Hospital
Date: Mon, 11 Mar 2002 08:36:21 EST
From: DocRickFry
E--
A couple of points
First--the MESS score is only meant to be applied to complex extremity injuries with combined vascular, skeletal soft tissue and nerve injuries--i.e. "mangled" extremities (see the title of Johansen's paper which introduced it)--it would be a misapplication to use it for the case example you gave.
Second--any nurse or yourself can find a shunt anytime of the day or night, unless you are operating in Rwanda. What is this preoccupation we have with only using commercial products that cost hundreds of dollars? Simple IV plastic tubing works just fine--run a segment through with heparin then stick in--I've used this many times and they work--even though it costs only pennies and does not come wrapped in a fancy package, believe it or not!
ERF
Date: Mon, 11 Mar 2002 10:52:23 -0600
From: ECThompson
Didn't the original post state that the patient had a large soft tissue injury to the proximal thigh? Why wouldn't MESS apply here?
E
Errington C. Thompson, MD, FACS
Trauma Surgeon
Trinity Mother Frances Hospital
Date: Mon, 11 Mar 2002 11:54:57 -0500
From: Frykberg, Eric
E--
Yes--MESS would be applicable for THAT case--but NOT for the example you proposed using it for--the uncomplicated stab to the thigh--don't mix apples and oranges. I, and the rest of the literature, agree, tho, that no scoring system is able to be used prospectively to make amputationdecisions by themselves. These systems are useful in noting those prognostic factors that should be used in individual casesto make the decision, tho.
ERF
Date: Mon, 11 Mar 2002 09:17:50 -0500
From: carl hauser, Department of Surgery, UMDNJ
ET:
I prefer Argyle straight shunts, but they're often not available because the elective vascular surgeons seem to like Sundt and Inahara shunts more these days. The Sundt works if they can find it, but in a pinch, a piece of IV tubing and a #1 silk will work just fine.
CJH
Date: Mon, 11 Mar 2002 11:57:13 -0500
From: Jeffrey Salomone
ECT-
We have a fair bit of experience with "damage control" shunting of mangled extremities at Grady. I agree with Eric's comments that shunts shouldn't be hard to find.
We have used Pruitt-Inahara shunts in the past and while some of my colleagues still like them, I have become disenchanted with them. They have a side port that you can transduce an arterial pressure from, plus two really cool balloons to help keep them in the vessel, however I am disappointed with their small caliber. We have had a few of these clot.
Argyle carotid shunts (the largest size in the package of 4) generally works well for a popliteal artery injury.
For other injuries (pop vein, fem art/vein, iliac art/vein, etc) we tend to use an approproate sized argyle chest tube trimmed to size (like a 20 F for femoral artery and 24 F for femoral vein). Because of the larger diameter, blood flow is excellent and I dont believe we have ever had one of these clot before our surgery to repair the vessels.
About 3 or 4 times annually we have a GSW victim arrive in essentially circulatory arrest from near exsanguination from a femoral GSW. While anesthesia begins resuscitation, we made an incision and shunt the injured vessel(s). Then close skin loosely with #2 nylon. Total time is generally less than 30 minutes from arrival in OR to being ready for transfer to ICU for continued resuscitation.
While our numbers are small, we believe this approach has resulted in saving both life and limb.
Jeff Salomone
Date: Mon, 11 Mar 2002 16:40:26 +0530
From: DR T I GEORGE
What about direct electrostimulation of the intact sciatic nerve
We have not been using intra-op stimulators and hence do not have them. As a substitute can we use electrocautery low intensity?
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.
Date: Mon, 11 Mar 2002 09:06:40 -0500
From: James Carr
My vote is to save. Do generous distal fasciotomies, watch myoglobin closely.
I'm not sure you can use the sciatic nerve electrical response as your main determinant. What if he has dense neuropraxia? The main issue is if trying to save his leg will do him in. It may, but initial response to Rx should help.
Jim Carr
Date: Mon, 11 Mar 2002 11:42:43 -0600
From: Adam Starr
I would vote for repair of the vessels in this patient. If he's stable under anesthesia, I think the best outcome will be obtained if he's able to keep his leg.
Adam Starr
Dallas, Texas
Date: Mon, 11 Mar 2002 12:45 pm
From: Bill Burman
Dr. George wrote: We have not been using intra-op stimulators and hence do not have them. As a substitute can we use electrocautery low intensity?
Jim Carr wrote: I'm not sure you can use the sciatic nerve electrical response as your main determinant. What if he has dense neuropraxia?
I once had a similar case assoc with a femur fracture. A crush injury from a forklift. The patient was intubated before neurologic assessment. There was a significant preliminary debate over whether to do amputation vs limb salvage (which contributed to warm ischemia time). The surgeons and anesthesiologists wanted amputation. Orthopaedics wanted limb salvage.
There was no nerve stimulator. The cautery was turned down low enough to stimulate but not burn local muscle tissue and then applied to the sciatic nerve. There was no response distally. Orthopaedics argued for a 30 minute trial of perfusion through a temporary shunt. The vascular surgeon agreed to a perfusion trial but insisted on a formal arterial repair while a four compartment fasciotomy of the lower limb was performed by orthopaedics.
30 minutes after reperfusion, sciatic nerve stimulation produced ankle/toe plantar flexion. Limb salvage was selected. To rule out a dense neruopraxia, the plan was to directly stimulate distal musculature through the fasciotomies.
The subsequent vasular repair/ORIF operation did not go well. Despite shortening the femur, reduction manuevers tore apart the femoral artery anastomosis. Another formal arterial repair was performed after ORIF.
Following this 4 hour procedure, the distal neurovascular exam was intact. However, despite regular, repeated debridements, within a few days postop the patient was septic and losing renal function secondary to myoglobin. A hip disarticulation did not save him. The limb salvage procedure was faulted in the trauma audit.
Date: Mon, 11 Mar 2002 15:24:51 -0500
From: Frykberg, Eric
The exact level of nerve function at the time of presentation of this complex limb injury is not as important as it was made in this presentation--the key is that the major nerve--sciatic, tibial, or two of the 3 arm nerves--is anatomically intact. Once that is determined and there is no other obvious indication for immediate amputation, the assumption of limb salvage should be made and revascularization completed-then observe the level of skeletal, soft tissue and neurologic function that is recovered over the next 24-48 hours. There is just no way of ever knowing what level of function a nerve has at this time beyond anatomic transection--I know of NO proven correlation of response to nerve stimulator to ultimate salvage and function--if anyone does, please provide it? It will always be no more than a guess, and we should all realize that.
Also--the Orthopedic literature is now very clear that many of the old neurologic criteria for limb amputation or salvage--like preservation or loss of plantar sensation--have since been proven fallacious, so be very wary of assessment of nerve function early on as the sole criterion for amputation--especially when it will never be any better than a guess with present technology.
There is a real problem with the team managing a patient like this when there is such disagreement over the need for amputation--the evidence for making this assessment is much better than that, but we have to know it, and be willing to be guided by data rather than the seat of the pants guesswork, which has a proven track record of being terrible for these injuries. Just to say "It needs amputation" or "it needs salvage" is no longer sufficient in 2002--hard and fast reasons--pros and cons--must be provided to support either stance. The level of evidence is not great, but a surprising amount is out there--certainly enough to give things 24-48 hours when the picture is not clear (as is most often the case)to sort out and see what you have. But again--unless perfusion is immediately restored and early --preferably prophylactic--fasciotomy liberally applied--you will be consigning the limb to loss no matter what. Don't begin discussing salvage vs amp until perfusion has been restored, if that is at all possible. And then--it is extremely important that the whole team--orthopedics, trauma, vascular surgery, rehab, phys Rx, plastic surgery nursing and--most importantly--the patient and family---ALL agree on the plan before proceeding. If this cannot be done, that is a signal that this team should meet and hash out a protocol in advance. They have a problem.
The key measure of success is what percentage of these limbs have gone more than 48 hours of salvage attempts (costly, morbid, prolonged hospitalization and time lost from work, fatal--YES, fatal! see Johansen's 1990 paper in J of Trauma where there were 6 deaths from complex extremity injuries due to flawed decisions to salvage) and yet get amputated, or are useless functionally, in the end anyway--each one of these cases represents a failure of appropriate decision-making, and should be discussed as a group to decide where they went wrong.
The generally agreed-upon criteria for immediate amputation at the time of presentation:
I think all of us realize that very few limbs meet these criteria for Primary Amputation nowadays.
ERF
Date: Tues, 12 Mar 2002 8:00 am
From: Bill Burman
Eric
>to say "It needs amputation" or "it needs salvage" is no longer sufficient in 2002--hard and fast reasons--pros and cons--must be provided to support either stance.
Your points are well taken about the need for more objective criteria for deciding amputation vs limb salvage with early reperfusion and liberal decompression fasciotomies - especially in borderline cases.
>The exact level of nerve function at the time of presentation of this complex limb injury is not as important as it was made in this presentation
In full recognition of the fact that the MESS score (J Trauma 30:568 1990): see is based on a 25 case retrospective and 26 case prospective study
Thus it looks like neuro status of the limb (which is a reasonably objective measure) is weighed pretty heavily in the MESS calculation. Nerve/muscle stimulation, which in and of itself has no more prognostic significance than "muscle contractility" is a crude attempt to get a sense of limb neuro status in the absence of a neurologic exam in order to compute the MESS score.
As stated in an earlier post:
"If this is rated as a "high energy" injury using a MESS score calculation , the MESS Score would be:
MESS Score > 7 - poor limb viability prognosis."
In other words, if you factor the MESS score into your decision making process in this case, it would favor an amputation if the neuro status is out and a limb salvage if the neuro status is intact. The scoring mechanism makes no specification as to whether nerves are in continuity or not, although in the article Johansen writes:
"division of the sciatic or posterior tibial nerve in adults results in an irretrievable peripheral neurologic deficit and patients with such an injury should undergo immediate amputation at the time of discovery of these injuries."
>most importantly--the patient and family---ALL agree on the plan before proceeding
If possible they should probably be informed about the following report from the OTA 2001 Annual Meeting (soon to appear in JBJS):
A multi-center, prospective, longitudinal study assessed the outcomes of 569 patients with severe lower limb injuries, with use of the Sickness Impact Profile (SIP) as the principle measure of functional outcome.
Conclusions: Patients with limbs at high risk for amputation but without risk factors predisposing to poor outcomes (i.e. lower level of education, non-white race, poverty, lack of private health insurance, heavy smoking, and involvement with disability compensation litigation) can be advised that reconstruction will usually result in a 2-year outcome equivalent to that of an amputee. This advice must be qualified to emphasize that this choice carries with it a higher complication risk, additional surgical procedures, and more hospital re-admissions. Efforts to improve the rate of successful reconstructions may have merit. Emphasis on reduction of complication rates, combined with a proactive modulation of patient risk factors known to influence outcome and targeted rehabilitation for workplace re-entry, could improve overall patient outcome.
>Skeletal and soft tissue damage is so great that repair is judged as futile Gustilo III-C injuries (altho labeled as such, the presented case was NOT a 3-C injury unless I missed something)
I think you may be reading the Gustilo Classification differently here:
"Grade IIIC - An open fracture associated with an arterial injury which requires repair."
Gustilo RB, Fracture Classification Manual, p 16, Mosby Year Book 1990 ISBN 0-8151-4047-9 or see Dave Templeman's (Ramon Gustilo's partner at Hennepin) OTA BFC Lecture on open fractures.
Bill
Date: Tue, 12 Mar 2002 10:05:40 -0500
From: Frykberg, Eric
Bill--
Thanks for these points,especially on the inconsistencies and inaccuracies of the MESS score, which are worthwhile clarifications of the issue--if you read the lecture you posted, the first slide emphasizes again the need for immediate reperfusion as the FIRST step, before any other assessment or judgements are made.
Another point I failed to mention is that vascular occlusion by itself will give very clear and strong neuro deficits indistinguishable from direct nerve injury--this is because nerve is the most sensitive tissue to ischemia, and gets knocked out very early when its blood supply is knocked off. This is another reason why assessment of neuro function BEFORE perfusion is restored is WORTHLESS as an indicator of neuro outcome, and should not be used to make an amputation decision. Within 6-8 hours, this function can be reversed with revascularization.
Finally--as to my understanding of Gustilo III-C injuries, your posted lecture confirms what I thought--that is, it refers to open, comminuted tib-fib fractures with vascular deficit. If this was not the original definition, that is certainly the convention currently used in the literature (I can refer you to any number of citations saying this), and obviously as well by your posted lecturer (who, as you note, is Gustilo's partner!).
He also makes another good point, tho--that is, that upper extremity complex injuries have entirely different implications with regard to limb salvage than the lower, and tib-fib injuries are very different (i.e. much worse) from thigh, for many good reasons, which is probably why tib-fibs are usually used in this context--it is with them that this dilemma is most likely to arise. Anyway--unless I missed something, the original posted case did NOT have a femur fracture, just severe soft tissue injury with an exposed but intact femur.
ERF
Date: Fri, 15 Mar 2002 18:07:37 +0530
From: DR T I GEORGE
Thank you for the interesting discussions especially from the OTA & AAST lists.
Now the follow up.
Our team decision was to attempt limb salvage.We had an informed consent for ablation from the relatives in case the events were not favourable.
Extensive debridement of the devitalised soft tissues were done. There was some retrograde flow from the distal femoral vessels. Both femoral vein and artery were reconstructed using long saphenous vein grafts from the opposite thigh. Fasciotomy of the leg were done for all the compartments. Now we were faced with the next problem. The soft tissue coverage for the vein grafts were inadequate. At this point of time patient was haemodynamically stable with good urine output. A latissmus dorsi muscle microvascular free flap along with split thickness skin graft was done to cover the vascular graft.
Patient was continued on ventillation post operatively. Inotropic support was required at this time. There was a gradual deterioration of renal parameteres and increased requirement of inotropic agents. Patient went on to oliguria with high coloured urine. There was a steady climb of cpk. At 36 hours a very high above knee amputation was done(Most of the muscles in the thigh which looked viable and were actively bleeding during the primary surgery were found nonviable now and only very little muscle could be salvaged). Soon after this the urine though small in amount became clearer. Patient was continued on ventillator, inotropic support and started on peritoneal dialysis. After the first cycle the electrolytes were maintained but serum creatinine was still high. The second cycle continued during which patient developed cardiac arrest from which he could not be resucitated.
There were a few events in the course which we could not quite understand: There was retrograde flow from the femoral vessels when we started. The leg compartments were quite soft when we started which kept on getting tenser later in spite of liberal fasciotomies, the flow back through the intact tissues laterally and posterolaterally in the thigh and also through the reconstructed femoral vein.
We do hope to get your comments on this case.
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.
Date: Fri, 15 Mar 2002 07:39:57 -0600
From: Steven Rabin
was there vascular injury more proximal? i have seen compartment syndrome of the gluteal area present with rhabdomyolysis and renal failure twice. Both were large individuals with a lot of muscle mass and had crush injury as well as their femur fractures.
Date: Fri, 15 Mar 2002 23:43:32 +0530
From: DR T I GEORGE
No. There was a good flow from the proximal femoral artery. In fact he was almost bleeding to death on arrival.
Dr.T.I. George