

Date: Tue, 28 Dec 1999 18:05:13 -0600
From: Doug Duncan
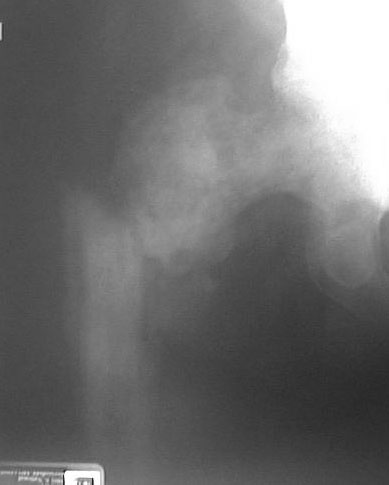
Subject: Subtrochanteric pathologic fracture
I am open to suggestions regarding the management of this patient'scomplicated problem.
| | |
This patient is a 61 year old with prostate ca metastatic to bone. Noapparent metastases to the liver, lungs or brain. Serum calcium isnormal. No apparent impending fractures elsewhere. He is on hormonetreatment for his prostate ca. He was ambulatory prior to falling inthe shower and fracturing his hip.
I've considered a Synthes IM rod with their proximal spiral locking blade forthe femoral neck with cement augmentation. One of my concerns with is reamingthe medullary canal without penetrating his very fragile appearing cortex thatmay be no firmer than the metastatic tissue in the medullary canal.
I'm also concerned about cut out of the fixation proximally. If I were toproceed with rodding, I would consider doing this as an open procedure using afemoral distractor for traction if necessary. This might allow me to injectcement more effectively and make it easier to convert to a prosthesis ifeverything falls apart.
The other consideration that comes to mind is a calcar replacing hemiprosthesis. However, the bone of the calcar may be very weak ornonexistent. Getting a secure attachment of the trochanter may bedifficult due to the soft bone from severe involvement of the bone ofthe trochanter and I would be concerned that it might not heal.
A hip nail with a very long side plate would be another option, but cutout proximally would be a worry as well as getting decent purchase ofthe of the screws for the plate.
Augmenting the fixation of either the plate or the rod with cement might be aproblem since there is not a discrete lytic lesion that can be curetted out andfilled with cement.
Any suggestions would be appreciated.
Doug Duncan MD
Date: Tue, 28 Dec 1999 22:09:05 EST
From: DGFWRIGHT
HowMedica makes a tumor replacement prosthesis..... modular, cementable .... agreat bailout .....consider having this in the room, as the things you'vementioned may be appropriate for a fracture without a tumor... but things alwaysget worse with cancer and the bone may not heal very well (if at all).
I would think the plan should be to get the patient up and walking - pain free... so perhaps this prosthesis would help.
Douglas Wright
Date: Tue, 28 Dec 1999 23:54:55 -0500
From: barrick
It looks like the entire head and neck of the femur are involved with tumor.So I would do some type of hemiarthroplasty replacement of the entireproximal portion of the femur---provided there is no involvement of thepelvic side of the hip joint.
E. Frederick Barrick, MD, Director of Orthopaedic Trauma, Inova Fairfax Hospital,Falls Church, VA
Date: Wed, 29 Dec 1999 08:52:31 -0700
From: John Ruth
I would not use the Synthes nail as there have been problems (
Date: Thu, 30 Dec 1999 13:00:21 EST
From: DoctorQ2
I agree with Dr Wright. A hemiprosthesis, although a larger exposure and longerprocedure, would allow the patient to walk the next day, as opposed to a longperoid of non weight bearing. Thus you would not have to worry about the bonequality. A proximal femoral replacement prosthesis would eliminate any questionof whether or not there is sufficient support of the calcar. Additionally, it isa much simpler procedure than it seems.
Louis Quartararo, MD; Johns Hopkins Bayview medical center, Dept of Ortho.; UMMS-shock trauma - dept of ortho.
Date: Thu, 30 Dec 1999 14:56:00 EST
From: anonymous
 |
Date: Thu, 30 Dec 1999 22:25:33 -0500
From: michael r. baumgaertner
The images on my screen are not adequate to assess the tumor's proximalextent. A CT scan may allay your fears of proximal fixation. I have foundthat the full length IM hip screw (34-42cm) works well for this pathologicprocess, and can be placed with a minimal surgical insult. The 18mm proximalnail expansion replaces the tumorous intramedullary contents and is anexcellent buttress, and the sliding screw seems to offer better & dynamicpurchase of the proximal fragment than interlocking screws, provided it isplaced dead center and very deeply.
Don't hesitate to use a joy stick tofacilitate the reduction and err on too medial an entrance site.A varus or significant extension deformity at the fx must be activelyprevented during entrance site preparation and nail insertion. The 10 mmdistal nail diameter is a draw back because it tends to float in the canal,so get it long enough and carefully guide it down the center. The 2.3 mm wallthickness makes it as strong as the delta recon system. A 12 mm version is dueout any time now, i am told. It probably helps to use tibial nail interlockscrews distally rather than routine 4.5 screws to increase the corediameter/fatigue life. No reason not to weight bear to patient tolerance. Inmy hands, cement would be counterproductive in a pt with reasonable lifespan.
mbaumgaertner