



Subject: Forearm non-union
Date: Mon, 28 Apr 2003 14:33:58 -0400
From: Kevin Pugh
Gentlemen,
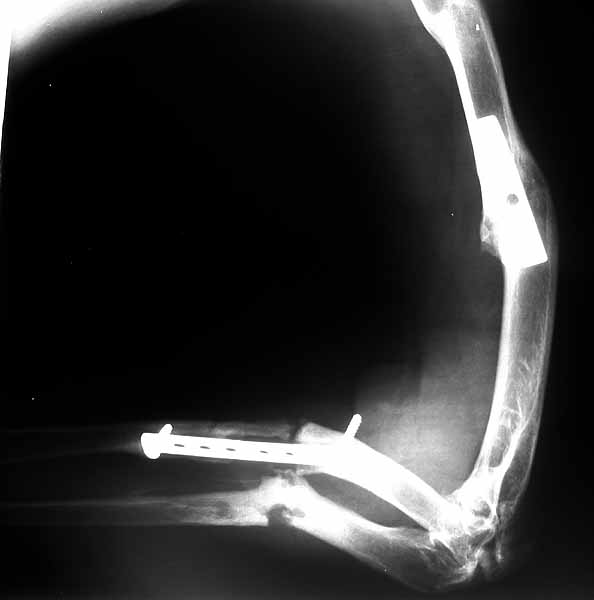
This is a West African man who was clubbed inthe forearm 2-3 years ago because he did not agree with the politics of the local rebels. The forearm and humerus fractures were open and treated surgically in his native country. He has since come to the US, sponsored by relatives, and is now seeking care for this problem. His soft tissue envelope is now closed and quite good. He did have some skin grafting on the forearm. His exam isintact in the hand, his shoulder is normal. He has almost no pronation and supination, and his elbow moves from 30-80 degrees. He has mild aching in the foream at night.
|
|
|
|
|
Suggestions? I have told him that we could make him more painful, and have quite a bit of morbidity, with no guarantees of improved function.
Kevin J. Pugh, MD
Chief, Division of Trauma
Department of Orthopaedics
The Ohio State University
Columbus, OH 43210
Date: Tue, 29 Apr 2003 19:55:12 -0500
From: Gregory J Schmeling
I would think that this would be very difficult. I think I would take radiographs of the opposite limb with mag markers to assess actual radial and ulnar length and compare them. I would assess the limb for chronic infection.If there remains near normal length of the ulna I would take it down and plate it to length. I would assess radial length and do a segmental allograft to restore length along with an open reduction of the radial head. If the ulna has lost bone I would shorten and plate it. I would then attempt to shorten the radius the same amount, do a segmental allograft if needed, and an open reduction of the radial head. Active infection makes this very difficult. The really difficult question to answer is whether the forearm will function or not and whether the above is a long run for a short slide. I am not sure how to assess whether reconstruction will result in function.
How much pain does he have? What is his current function? Dominant limb?
Gregory J Schmeling
Orthopaedic Trauma
Medical College of Wisconsin
Date: Thu, 1 May 2003 13:06:13 +0600
From: Alexander Chelnokov
Hello Kevin,
KP> This is a West African man who was clubbed inthe forearm 2-3 years
[...]
Suggestions? I have told him that we could make him more painful,
and have quite a bit of morbidity, with no gaurantees of improved
I would suggest this is a case what the Ilizarov technique is developed for.
I would mount something with hinges with separate control for radius and ulna, corrected axis and length of both bones, restore relations in the distal RU joint and then re-estimate what to do next. Possible optins would be resection, bone grafting, conversion to IM nails, maybe something else.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Thu, 1 May 2003 09:10:28 -0400
From: James Carr
I'll put in my two cents, if a little crazy. You can always make a condition worse, but I think this guy has a lot to gain. I would first plate the ulna with a long 3.5 mm DC plate, and bone graft. I then would do a long Thompson approach to the radius, with the main idea to find the radial nerve first. I would think that is his major risk. You should be able to expose from the elbow joint to however distal you need. I then would see how much radius I needed to shorten to get the radius back in place. I would plan on some type of posterolateral elbow stabilization as described by Morrey et al. I think shortening makes more sense than trying to lengthen. The radius can then be stabilized with a 3.5 mm DC plate. As a last resort, the radial head could be resected, but I'll bet it goes back in with the right amount of shortening.
Jim Carr
Date: Sat, 3 May 2003 15:46:57 +0600
From: Alexander Chelnokov
Hello James,
JC> I'll put in my two cents, if a little crazy. You can always make a condition worse, but I think this guy has a lot to gain. I would first plate the ulna with a long 3.5 mm DC plate, and bone graft.
Do you suppose that acute open correction is tolerated better? To our experience, whatever one uses for definitive stabilization, if length and axis were preliminary restored by gradual bloodless technique it makes main stabilization procedure much easier technically and less invasive. So it may influence positively the functional outcome.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Sun, 4 May 2003 08:33:06 -0400
From: James Carr
Alex
There is no doubt in my mind that Ilizarov is the best overall technique to handle these types of problems. As one who does not possess those skills, I have to "live by the sword, and die by the sword". In my case that is plating/nailing. Plating involves a much larger dissection, and risk of heterotopic bone, N/V damage, etc. That's why I suggested shortening, which may or may not be needed, but puts less tension on scarred tissues. I admire the skills of those like yourself facile in Ilizarov technique, but feel I have a tough enough time mastering "traditional" fixation techniques.
Jim Carr
James B. Carr, MD
Palmetto Health Orthopedics
Date: Sun, 4 May 2003 23:46:19 +0600
From: Alexander Chelnokov
Hello James,
JC> possess those skills, I have to "live by the sword, and die by the sword". In my case that is plating/nailing.
Frankly speaking the skills are rather simple, and it can be just useful addition to plating/nailing.
JC> puts less tension on scarred tissues.
Exactly what is addressed by the Ilizarov...
JC> I admire the skills of those like yourself facile in Ilizarov
I'll show this line to my wife.
JC> but feel I have a tough enough time mastering "traditional" fixation techniques.
I still attach a couple of images as Bill Burman requested an example of how the frame should be applied. The only similar case i quickly found is the one with Madelung deformity with chondroma of the distal ulna, where its resection was performed along with perQ osteotomy of the radius, with gradual restoration of the axis. In the discussed case a very close assembly can be used.
 |
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Fri, 09 May 2003 15:10:35 -0500
From: Djoldas Kuldjanov
Hello Kevin,
In reviewing this case my inclination is to osteotomize the ulnar nonunion, shorten and plate it. The difficult part will be deciding what to do with the radius. The radial head has been out for some time now and I question the condition of the elbow joint. Can the proximal radius be shortened reduced and plated? Should it be excised (possibly gaining more elbow joint motion) or does it require a radial head replacement after excision?
If you are still considering what to do with this case, it might be worth while to obtain a CT scan of the elbow and forearm with 2mm cuts for further evaluation. As you know I have the ability to make a 3-dimensional model from the CT scan that could be helpful in preoperative planning. If you are interested, send me copy of CT on CD-ROM. Usually the X-ray technician can put the study on CD.
Djoldas Kuldjanov, M.D.
Dept. of Orthopaedics
St Louis University
{kind=link}