




Date: Mon, 4 Dec 2000 14:37:50 -0500
Subject: Sacral "H" Fracture
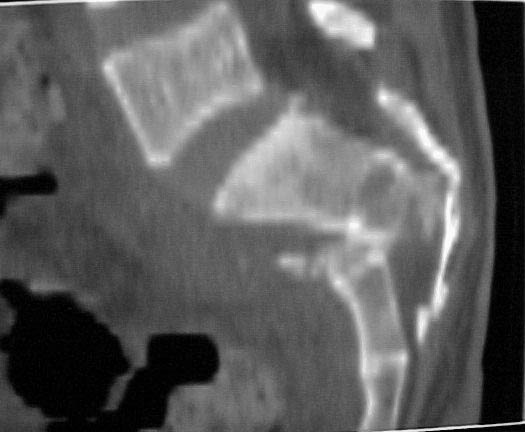
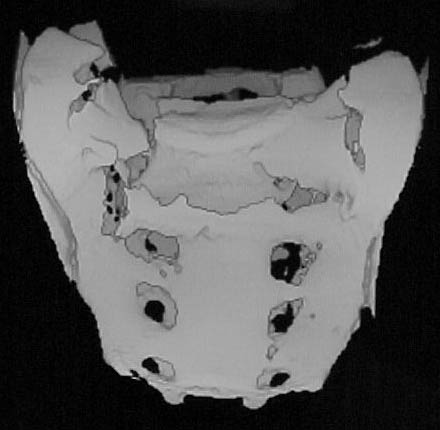
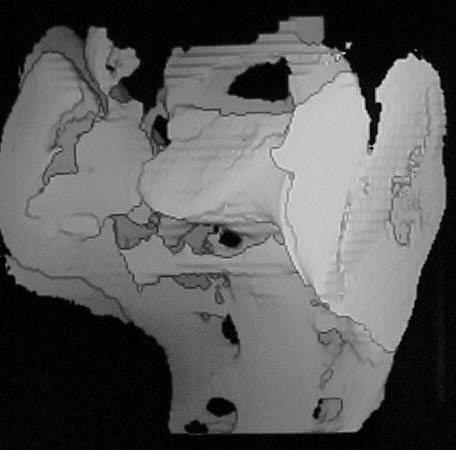
A 28 year old male jumped from the 4th floor on 11-25-2000 sustaining an L1 burst fracture that has been fixed anteriorly by the neurosurgeon with a strut between T12 and L2. A Kaneda device was placed anteriorly as well. My concern is the pelvic ring injury. There are bilateral sacral fractures through the foramen and a transverse element through the sacrum between S2 and S3. the lower part of the sacrum is displaced forward. Anteriorly there are right superior and inferior pubic rami fractures.
He also has bowel and bladder sxs. The neurologic injury could be from the L1 burst or from the sacrum or both.
My question is operative treatment or not for the pelvic ring injury. If operative; how does one approach the fracture (anterior or posterior); how does one reduce the fracture and what fixation?
What would happen if left alone and just monitored for further displacement?
Paul Koerner
|
|
|
|
|
Date: Mon, 04 Dec 2000 21:26:09 -0800
From: Carlo Bellabarba
This is a difficult problem. I would be aggressive with this fracture, both in terms of stabilization and of decompressing the terminal portion of the cauda equina. A good decompression would require a reduction of the transverse sacral fracture, since the displacement/shortening of the transverse sacral fracture is tenting the sacral roots. The technique we've been using here at Harborview for this type of injury, pioneered by my colleagues Chip Routt and Jens Chapman, is a combination of iliosacral screws and fixation from the lumbosacral spine to the ilium. If they're out there listening, their expertise will surely be of help to you. This "combination" technique allows you to stabilize both the vertical and transverse components of this fracture. The iliolumbar part of the procedure consists of the following sequence:
The advantages are excellent stabilization and a decompression which is second-to-none. Obvious disadvantage is long operation which can be tricky and has a bit of a learning curve.
Date: Tue, 05 Dec 2000 08:26:11 -0800
From: Chip Routt
Thanks, these are relatively uncommon injuries with a variety of presentations.
 |
 |
 |
Longitudinal Fractures |
Central Fractures |
Transverse Fractures |
In "U-shaped" sacral fractures, the cervico-thoracic-lumbar-upper sacral component behaves as a unit, while the caudal sacrum and remainder of the ring function as a unit...not really a pelvic ring injury...more analogous to an "upper sacral traumatic spondyl-olisthesis/-optosis". These may be missed initially. A high suspicion index is helpful, and the screening AP pelvic radiograph reflects a "paradoxical inlet" appearance to the upper sacrum when there is deformity. A lateral sacral view is usually diagnostic.
The neuro exam is variable, but usually reveals some abnormalities. Local degloving injuries are not uncommon.
In "Y-shaped" sacral fractures, the "U-shaped" sacral injury is complicated by an additional associated hemi-pelvic ring injury, which may or may not be unstable...best understood as the "U" component plus ramus fractures anteriorly and a unilateral fracture continuation of the "U" caudally thru the sacrum sagittally...therefore, potentially more instability for the clinician to deal with - upper sacral and hemipelvic combined instabilities.
"H-shaped" sacral fractures are the combination of a "U" with associated bilateral pelvic ring injuries...analogous to a "Y" with associated bilateral ring injuries...fortunately, rarely are both hemi-pelves clinically unstable.
Also, please note that the caudal sacral component is not displaced anteriorly...this is the stable component of the sacral injury which remains attached to the uninvolved portion of the pelvic ring. The spinal segment is the unstable/displaced component.
Realize that the cervico-thoracic-lumbar-upper sacral segment is the unstable and displaced component.
Your patient's injury mechanism is common.
These patients have other-level spine injuries, as well as the typical injuries associated with significant falls...so, rule them out in some manner.
Several questions still remain:
1. What is the physical exam of your patient's pelvis? Is there instability to exam? Did you examine it under fluoroscopy/anesthesia in the OR at the time of his neurosurgical operation? (Usually the best and most revealing exam.) If so, was it unstable, and if so, at which pelvic sites of injury? Where are his surgical wounds? Are there associated pelvic/lumbodorsal soft tissue injuries? What is his peripheral neurological exam, specifically?
2. If his pelvic ring is unstable and untreated, why did he have a neurosurgical operation several days ago without some form of pelvic ring stabilization?
3. Do you have additional images that you could share? It would be very helpful to see such images in order to specifically identify the injury.
4. May we see the lumbar reduction and fixation construct?
Thanks-
Date: Tue, 5 Dec 2000 18:39:01 -0000
From: Chris Oliver
We had similar very case in Edinburgh recently. Fall 50ft. From bottom up: Bilateral Calcaneus, Bilateral Tibial plateaux (2 and 6+: nasty soft tissues), H fracture of sacrum (just like case shown), Undisplaced fracture both sup+inf pubic rami, 30% wedge compression L3 involving middle column, Thoracic wedge fracture, closed humeral shaft. CT abdomen (moderate retroperitoneal haematoma only), cysto-urethrogram and pelvic angio negative. No peripheral neuro or bad pelvic soft tissue injury. Initially immediately treated with anterior pelvic x-fix. as EUA was unstable (but not grossly). Patient currently has ARDS at 2/52 post injury. Have decided not to fix spine or pelvis. Is being treated with anterior frame for the present. Will now leave frame on for 8/52.
To stabilise sacrum H fracture without doing L3 would make stability of either fixation compromised. Logically would fix sacrum and spine in one sitting but this would be massive surgical exposure and potential biomechanically unstable fixation. Sacral fixation is just not possible to guarantee adequate fixation, even putting rods out into the ilium is going to not give stability with a long lumbar fusion. Last experience in Edinburgh was massive uncontrollable coagulopathy trying to stabilise H sacral fracture and spine at the same sitting. Very nasty injury.
Date: Tue, 05 Dec 2000 13:59:01 -0600
From: Adam Starr
Mr. Oliver,
Initially immediately treated with anterior pelvic x-fix. as EUA was unstable (but not grossly)...Will now leave frame on for 8/52.
Now THAT's interesting. I've never been able to figure out how you distinguish "gross" vs. other forms of pelvic instability. I figure that if I can wiggle it with my hands, it's unstable. Was it unstable on fluoroscopy? How much motion did it show?
Also, was the anterior ex-fix frame placed to address hemodynamic instability? I don't guess you meant it as a treatment for the posterior ring injury?
Thanks,
Date: Tue, 5 Dec 2000 22:35:04 -0000
From: Chris Oliver
Gross v stable is difficult to objectively measure, perhaps Chip can tell us what is gross and what is subtle? How do you measure instability with fluro objectively?
Frame was put on for haemodynamic instability initially but now will be definitive treatment. It cannot possibly treat the posterior injury.
Date: Tue, 05 Dec 2000 15:30:29 -0800
From: Chip Routt
OK.
Unstable pelvic ring disruptions demonstrate movement on manual examination. The noted movement is unique for each patient (and perhaps examiner) and is dependant on numerous factors. The exam produces pain in most patients. If the patient is under anesthesia, the exam does not cause pain, and the fluoroscopy provides visual information regarding the sites of pelvic injury, and their individual contributions to the overall pelvic ring instability...sometimes the visual info is impressive. This tactile and visual information is then used to formulate a strategic management plan.
Keep on working.
Keep on thinking.
Good luck-
Chip Routt, M.D.
Date: Wed, 6 Dec 2000 11:01:30 -0500
From: Koerner, Paul MD
Chip-
Further images included.
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
Spoke with Gary Gruen at Pittsburgh who is just decompressing the sacral nerves without fixation or reduction. Claims to have the second largest series. 50% get better with decompression. 25% get better away without decompression. With surgery appear to improve slightly.
Thanks for educating me about this lesion. I'm sure that I have missed a couple in my career. I won't miss any more. The concept of the spine disconnecting from the pelvis is wonderful. The concept of the spine going posterior rather than thinking of the distal sacrum as going anterior helps conceptualize the real pathology. Kind of like AC joint separations where the shoulder drops down rather the clavicle going up.
The Y component (right hemipelvis lesion) is stable. What do you think of just decompressing the nerves as suggested by Dr. Gruen and keeping the patient bed to chair for three months.
Date: Wed, 06 Dec 2000 09:26:16 -0800
From: Carlo Bellabarba
The concept of the spine disconnecting from the pelvis is wonderful. The concept of the spine going posterior rather than thinking of the distal sacrum as going anterior helps conceptualize the real pathology.
That is precisely why connnecting the lumbosacral spine to the pelvis (eg. with iliac screws) does, in fact, stabilize these injuries.
Date: Thu, 07 Dec 2000 07:27:38 -0800
From: Chip Routt
i don't remember reading his series, and cannot find it in the literature. where are these results published? i need that reference please.
i disagree with decompression alone, and bed-to-chair mobility without some support for this injury...remember, this is an unstable situation at the upper sacrum, and potentially the ring!
chip
Date: Thu, 7 Dec 2000 10:51:50 -0500
From: Koerner, Paul MD
Chip,
Here is the reference:
http://www.hwbf.org/ota/am/ota97/otapa/ota97707.htm
The patient and family are deciding on operative vs. nonoperative treatment. We are considering transfer to you. I spoke with Carlo yesterday and I understand that he and Jens are going to Davos.
I agree that people tend to do what they know. When one asks for advise one is usually looking to confirm ones own thoughts on the matter. One doesn't want to hear otherwise. If that's ones attitude then why bother to ask. I notice at conferences I tend to go the topics that I already know and avoid going to areas that I don't know. I am changing now that I realize this. I have learned quit a bit about this injury now and have you to thank. Life is not a competition. We are in this together. We are all one and all go through the same life struggles. Why not help one another.
Thanks,
Paul
Date: Thu, 07 Dec 2000 19:36:07 +0000
From: bruce meinhard
well said...amen! otherwise we would sound like lawyers wouldn't we?
Peter Carter in Texas said, "If you always do what you always did, you will always get what you always got."
Date: Tue, 13 Mar 2001 10:48:36 -0800
From: Chip Routt
How about (for a change) some 3 months follow up information ?
Chip
Date: Wed, 21 Mar 2001 12:29:24 -0500
From: Koerner, Paul MD
Speaking with the patients father - patient went to the Miami Project at Jackson Memorial Hospital. They tried over two hours to reduce the sacral fracture without success. They felt it was too risky to rebreak the sacrum and force the reduction. They decompressed the nerves and removed the deformity. They rejoined torn sacral nerves using a new technique involving living tissue glue. Patient is currently walking with a walker.
Paul
Date: Wed, 21 Mar 2001 12:15:41 -0800
From: Chip Routt
Wow. Tissue glue.
Why did they wait for it to heal before attempting reduction?
I hope he makes progress.
Thanks for the follow up.
Chip
Date: Wed, 21 Mar 2001 12:42:04 -0800
From: Carlo Bellabarba
In such cases, a reasonable alternative to obtaining a reduction is to mobilize the roots (easy when they're torn) and burr down the posterior sacral bodies to decompress the canal and perform a "kyphectomy", of sorts.
Since this is a sacral root level injury, I certainly hope he can walk with a walker. (I forgot whether his simultaneous thoracolumbar injury had an associated neurologic deficit). I'd be more interested in knowing what his bowel and bladder function is like.
Carlo Bellabarba
{kind=link}