



Date: Wed, 12 Apr 2000 09:21:05 -0700
Subject: Pilon Fx
From: Issa AbuRiziq
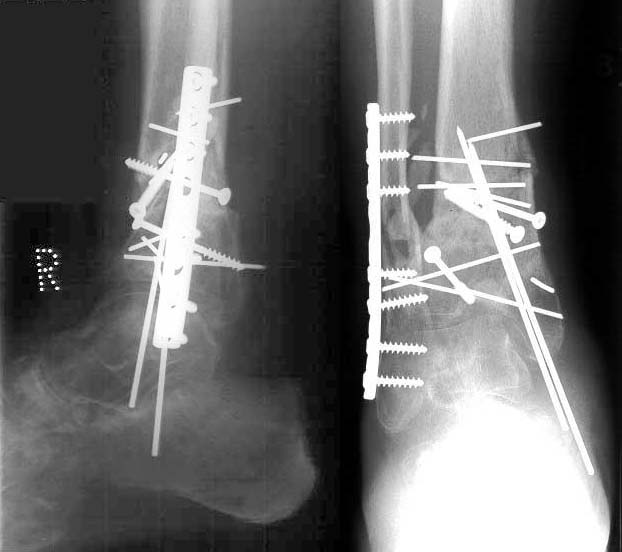
60 ys old man hit by a van 11 months ago. Sustained a compound (Grade 2 Gustilo - over lateral malleolus) Pilon fracture of the Right ankle. Treated by ORIF + wound debridement + partial closure.
|
|
|
|
Developed deep wound infection with Staph Aureus and Pseudomonas in January 2000 treated successfully (now CRP and ESR back to normal) wound fully healed now.
When last seen was able to PWB and had +/- 30-40% general stiffness of the ankle- less stiffness in the subtalar joint. Has moderate pain on weight bearing. Currently having physiotherapy with the aim to reduce stiffness and pain and improve walking and increase weight bearing. More up-to-date Xrays and current complaints and current findings on examinations will be posted soon.
 |
Any comments and opinions from members of the group?
Issa AbuRiziq - Locum Consultant Orthopaedic Surgeon at Monklands
Hospital - Airdrie - Scotland - UK.
Date: Wed, 12 Apr 2000 06:21:17 -0500
From: Adam Starr
I would not have ORIF'd the open pilon fracture. I would have treated him in an external fixator spanning the ankle, after an I & D. I would have I & D'd him again after 48 hours, and every 48 hours until his lateral wound was closable.
Once the skin wounds were healed and dry, say in 2-3 weeks, then I would address the joint surface, if necessary, with ORIF.
It might have been possible to get a reasonable reduction of the joint simply with distraction using the ex-fix.
I don't think that k-wires and isolated screws are adequate to hold reduction on the medial side, unless you supplement them with a medial ex-fix.
The distal tibial articular surface above the medial "shoulder" of the talus is impacted still. He'll wind up with arthritis there.
I think your best bet is to leave him as he is. If he develops post-traumatic arthritis, I would do an ankle fusion.
Adam Starr, Dallas
Date: Wed, 12 Apr 2000 11:19:03 -0700
From: Thomas A. DeCoster
Although there are times when unusual approaches are best for an individual situation, the radiograph shown from May 1999 which shows two long incisions and multiple screws and Kwires around the distal tibia is similar to examples I have seen presented in lectures entitled "How Not to do AO Technique". One must be very careful to avoid excessive soft tissue dissection in the pursuit of "anatomic reduction" especially in distal tibia fractures. The risk of excessive dissection must be balanced by the gain in stability which is not often achieved with multiple screws and Kwires. Whether this is the unfortunate result of an attempt at "AO technique" or the unfortunate result of promoting "alternatives to AO technique" or something else, I'm not certain.
Ankle fusion if (probably) and when (hopefully at least a few years) needed might be helpful in the future management of this patient.
tdecoste
Hello Thomas,
I agree fully with all what you say. However the fracures have united now and there appears to be no active infection. Is there any thing we can do before a fusion?
ISA
Date: Wed, 12 Apr 2000 15:47:56 -0400
From: William Obremsky
He appears to have an incongruous joint. I would offer him an ankle fusion. At 60 yo this should give him a functional painless limb.
Bill Obremskey MD MPH, University of North Carolina
Date: Thu, 13 Apr 2000 05:40:53 -0700
From: ISA
I think eventually we will have to offer this patient a fusion.
ISA
Date: Thu, 13 Apr 2000 09:10:18 +0600
From: Alexander Chelnokov
Well it was a good example against this sort of ORIF and for closed ex-fix or ex-fix with limited internal fixation for similar cases. For now i don't see any reasonable options of long-term positive effect except hardware removal (maybe partial) and ankle arthrodesis with axial correction. I would prefer ex-fix for this.
Best regards,
Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics, Ekaterinburg 620014 Russia
Date: Thu, 13 Apr 2000 05:35:32 -0700
From: ISA
Hello Alexander,
If I can treat this fracture again from the start, certainly I would treat it differently now. I would use an ExFix+minimal internal fixation. However I am fairly sure the fractures have united now. The defect in the articular surface on the medial side I believe is causing the varus deformity. Perhaps the two Kwires which have migrated are stopping the development of more varus. I plan to remove them and see what happens?! What about a corrective osteotomy?
Best regards.
ISA
Date: Thu, 13 Apr 2000 16:09:15 +0600
From: Alexander Chelnokov
Thursday, April 13, 2000, 6:35:32 PM, you wrote:
it differently now. I would use an ExFix+minimal internal fixation. However I am fairly sure the fractures have united now.
Union itself is not a problem for epimetaphyseal fractures.
migrated are stopping the development of more varus. I plan to remove them and see what happens?!
I don't think any measures can improve the joint congruity.
What about a corrective osteotomy?
AFAIK ankle fusion has the same or better results comparatively to reconstructive surgeries which finally result with joint stiffness and pain. So maybe better to perform definitive surgery, but axial correction along with the fusion i presume to be essential not to harm subtalar joint.
Best regards,
Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics, Ekaterinburg 620014 Russia
Date: Thu, 13 Apr 2000 06:53:26 -0500
From: Adam Starr
I would do what you're doing - try to improve function with physical therapy, and alleviate pain with NSAID's.
I wouldn't operate on this patient again (except maybe to remove hardware) until arthrodesis is required.
Adam Starr, Dallas, Texas
Date: Thu, 13 Apr 2000 11:56:55 EDT
From: Tadabq
regarding distal tibia fracture now 8 months post injury with some articular incongruity and the talus settling in to what appears to be a defect or depressed area of the medial plafond.
although I have seen this problem many times I am not aware of any reports of successful joint salvage through further surgery. Intra-articular osteotomies are very difficult and risk soft tissue problems making the patient worse. The lateral border of the tibia shaft lines up with the middle of the talus so this deformity is not only the medial plafond defect.
I would consider aggressive nonoperative treatment in the form of ankle range of motion and proprioceptive training. shoe modification in the form of arch support and ankle support and rocker bottom sole. The patient result does not entirely correlate with the radiographic appearance as I have seen patients with even worse xrays functioning reasonably well. I would hold off ankle fusion until patient symptoms clearly dictated it.
tdecoster