

Date: Mon, 3 Mar 2003 08:03:52 -0700
Subject: High Velocity GSW to leg
From: Thomas Higgins
List-Server members:
Attached are the pre and post debridement radiographs of the L leg of a 47 y.o rancher flown in (to Univ of Utah) from Wyoming. Very close range, high velocity round to leg (.22-250, which the ranchers use mostly to shoot coyotes). Dips Copenhagen, no other medical issues. 6'2", 225 lbs. Spends most of his day on and off horses and working the ranch.
|
|
Plantar sensation present. No dorsal sensation. 2+ palp pt,doppler signal in dp is retrograde flow. Anterior compartment, lateral compartment, and half of deep posterior compartment gone. Clinical photos not available at this time (photocard reader won't work right now).
Defect is Lat Dorsi sized, with very healthy appearing stump of A-Tib available. Bony defect (when measured vs. contralateral radiographs) is between 6 and 7 cm.
Hard working man, supporting a family, if he doesn't work, he doesn't eat. We discussed bone transport, how long salvage would take, and the leg he will have afterward. I have also offered amputation.
I would appreciate any opinions / feedback, etc...
Thank you
Thomas Higgins
Date: Mon, 3 Mar 2003 11:39:59 -0500
From: Jason Nascone
Tom
Even with salvage there a good possibility of the leg not functioning in the capacity he needs. Not to mention the time of transport, potential docking problems and over all injury to soft tissue envelope. My vote is for amputation and allow him to move forward.
Jason Nascone
Washington DC
Date: Mon, 3 Mar 2003 22:30:35 +0530
From: DR T I GEORGE
Dear Thomas Higgins
If you have the expertise available I would suggest the following:
1) Convert the ex fix to a solid nail with interlocking.
2) Cover the wound with vascularised muscle flap and bone. Suggest Latissmus
dorsi and contralateral fibula.
If conditions permit it can be done in one stage.
We have done vasularised fibula with Ilizarov fixator when conditions were not favourable for internal fixation. Saves a big headache of bone transport.
DR T I GEORGE.
Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular and Hand Surgery Unit,
Metropolitan Hospital,
Trichur. South India
Date: Mon, 3 Mar 2003 11:14:51 -0800
From: Chip Routt
You have many options.
It's good to remember tetanus status, IV antibiotics, debridements (you've really got a debridement there!), and irrigations.
With a viable sensate foot, most wouldn't advocate amputation.
Sometimes we forget that the limb can be shortened a bit to help both osseus and soft tissue "issues"...so at least consider it and its impact.
Without seeing the traumatic wounds/etc, it's difficult to make a good comment.
Given the films and his life scenario, I'd convert from the frame to a medullary locked tibial nail and strongly consider fibular stability. If you had the tibial fragment that you removed, it really helps for length and alignment during nailing...then remove it immediately after nailing/locking if it's non-viable.
The defect would do well with antibiotic-beads, particularly around the tibial bone ends.
The soft tissue coverage would be based on the wounds, and left to the judgement of the expert...hopefully early coverage of some sort.
Exchange the beads in 6-8 weeks for graft...I'd grind cancellous allograft with some of his and make a dense paste to pack particularly the ends with, and fenestrate the ends with a drill.
I don't think he needs to "give up the Cope", but it sure wouldn't hurt...but, good luck on that.
He'll need some friends to help with the cattle/etc for a while...hopefully he has some family/friends to help.
Maybe the "ring and transport experts" will comment.
Let us know what you choose.
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
Seattle, WA 98104-2499
Date: Mon, 3 Mar 2003 13:01:26 -0700
From: Johh Ruth
Tom
I would agree with the IM nail plus beads plus flap coverage. You will need to splint the foot in neutral to prevent equines contracture. Once the soft tissues have healed you can lift the flap and remove the beads and consider corticotomy with transport over the rod or massive ICBG plus helper (allograft) as suggested by Chip. Regardless of method, he is in for about a year of treatment.
Date: Mon, 3 Mar 2003 16:32:57 -0500
From: J. Tracy Watson
Depending on the availability of soft tissue coverage will help determine the treatment....if it's flappable then go with the IM nail etc etc as has been previously mentioned.....If soft tissues a mess but foot is viable....I would place in an Ilizarov frame and do as much acute shortening as soft tissues allow....acutely shorten in OR with a doppler....gradually shorten until you get a decrease in the doppler signal and then distract out until signal is strong and clear...usually this recruits enough soft tissue that the wounds will close by 2nd intention and granulate to extent all you need is a skin graft after about 10 days....this shortening vastly decreases the transport time...you do a proximal corticotomy and then transport any residual distance to achieve docking ..... continue to lenghthen thru healthy bone...the advantage of this is that you get a healed docking site quickly...and can stop the lengthening process at any time if the guy gets a little frame psychosis.....however since this guy is from WYO...chances are I know him or his family....and he won't complain,,,he'll continue to work with his frame on and be the model of compliance and good manners.....like all good ole boys from WY.......
Date: Mon, 3 Mar 2003 12:29:50 -0700
From: Thomas A. DeCoster
Regarding case of 47 yo male with post-traumatic segmental bone defect of the left tibia and fibula shaft from a gun shot.. Patient has good arterial supply to the foot, plantar sensation intact, absent dorsal sensation, gross loss of muscle in the leg, no other injuries and no other medical problems.
His initial treatment is irrigation, debridement (etc) and external fixation at normal length.
Treatment options start with amputation versus salvage. Salvage options are many. The bone defect can be managed with cancellous bone graft, structural graft (free fibula or other), bone transport. Augmentation techniques include OP1 (BMP) and other biological stimulants, various bone graft alternatives (allograft, synthetic graft, coral), cages, synthetic scaffolds, stimulation (electrical, ultrasound, other).
In this case the adjacent fibula also has a 6 cm defect.
I would consider salvage as preferable to amputation, even though it may take 1-2 years of treatment and perhaps $100,000.
I have managed a similar case with acute shortening then lengthening. There is no donor site morbidity and nothing lost if amputation required. Acute shortening compensates for the soft tissue defect so you won't need a free flap to get coverage. The fracture can start to heal right away instead of waiting for the transport segment to dock. Massive cancellous grafting with this defect is very slow to incorporate and the ultimate bone isn't always strong and the donor site morbidity is significant. This approach also allows sequential decisions over time as he adapts to the realities of this situation.
The new augmentation (OP1 etc) and synthetic scaffolds techniques are appealing but aren't powerful enough on their own for this much defect. Free fibula isn't strong enough.
Tom DeCoster
Date: Tue, 4 Mar 2003 02:43:26 +0500
I also vote for bone transport over the IM nail after soft tissue coverage.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 3 Mar 2003 23:55:33 EST
From: Aobonedoc
Tough case.
With anterior, lateral, and part of deep post compartments gone, even healed bone without infection may leave with a significant deformity in the foot which will compromise final outcome.
Personally, for me, I would take an amputation.
If salvage choosen, would consider nail covered with free flap, perhaps antibiotic calcium sulfate beads (I have used three times, not FDA approved) with delayed grafting later.
Sincerely and respectively,
M. Bryan Neal, MD
Arlington Orthopedics and Hand Surgery Specialists, Ltd.
Arlington Heights, Illinois 60005
Date: Mon, 3 Mar 2003 14:48:13 -0800
From: Chip Routt
Anecdote for single bone grafting, only FYI-
 |
Here's an example of a 30s yo male patient with a similar (but "tibial only") open segmental defect after a motorcycle accident, treated with nailing, several I&Ds, defect beads, closure/coverage, then a single allo-auto(combo)grafting @ 7 weeks after injury.
We anticipated union problems so we used a small diameter hollow nail, and left it available for easy exchange...but never needed to.
These films were taken 8 months after injury. You can see where the defect was. But, he did have fibular support.
Maybe he's just real lucky.
Lucky is a good way to be-
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
Seattle, WA 98104-2499
Date: Tue, 4 Mar 2003 11:47:50 -0700
From: Thomas Higgins
Thank you to everyone for your input / suggestions / feedback.
With regards to the degree of bony debridement , I think the presentation film was deceiving. The limb was foreshortened in the field splint, and I believe that any "large" pieces of tibia are in a Wyoming pasture. His length as set in the frame was based on the contralateral limb.
I am not really comfortable with transport over a nail given that coronal split that runs right up into the metaphysis.
Dr. Watson, your name did not come up, but he certainly seems to be a "WYO good ole boy".
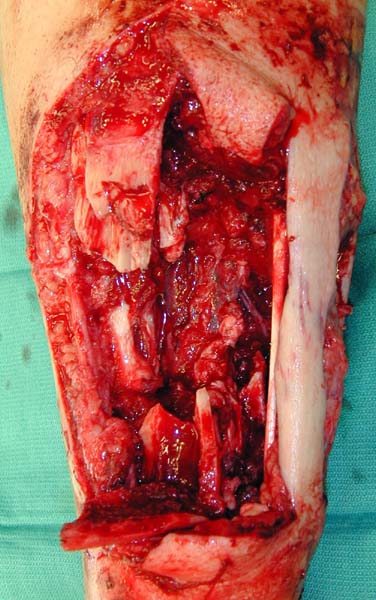
I have attached the clinical photos which were missing yesterday
 |
 |
 |
 |
Date: Tue, 4 Mar 2003 17:50:07 -0600
From: Sciadini, Marcus
Tom:
I wasn't able to download the images, but based upon your description would tend to agree with Jason. Another option, favored by Dean Cole in these cases, is acute shortening, IMN, soft tissue coverage and transport over a nail. It might make limb salvage with transport a more functional option than classic Ilizarov.
Marcus