

Date: Tue, 25 Feb 2003 00:53:51 +0530
Subject: Tibia Fx - Comminuted Supramalleolar - Open
Friends,
I present this case for opinion on management.
Middle aged adult was injured while travelling in a train(accidentally put his leg out). Presented with injury to left lower leg. Lacerated wound over the fibular fracture. Also another wound over the foot anterolaterally. No deficits.
On day one wound debridement followed by calcaneal traction done. Needs further stabilisation and a small split graft laterally. At present the fragments are putting pressure on the anterior skin. Will be happy to get your opinion on possible methods of stabilisation.
|
|
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.
Date: Mon, 24 Feb 2003 13:44:32 -0600
From: Obremskey, William T
I&D wounds
ORIF fibula w/ 1/3 tubular plate
Internal fixation of medial tibia w/ perc plate or ORIF if perc plates not available.
Bill O
William T Obremskey MD MPH
Vanderbilt University
Orthopedic Trauma Division
Nashville, TN
Date: Mon, 24 Feb 2003 19:47:25 -0000
From: Chris Wilson
Either hybrid external frame( ring with wires through metaphysis and unilateral pins in diaphysis)with plating of fibula or full ilizarov frame. Severe comminution-would bone graft be a good idea?
Chris Wilson
University Hospital
Cardiff UK
Date: Mon, 24 Feb 2003 14:40:55 -0600
From: Adam J. Starr, M.D.
Hi Dr. George.
I agree with the wound debridement. I would continue antibiotic coverage, and then I would put an ankle bridging external fixator on the patient's leg. Get the best reduction you can with the fixator. Keep it there until the soft tissue envelope was ready for definitive fixation. This will likely take 2-3 weeks.
Good luck.
Adam Starr
Dallas, TX
Date: Tue, 25 Feb 2003 09:42:33 +0200
From: Anton V. Vladzimirskiy
We have a lot of patients with similar traumas. Treatment: 1) Debridgement 2) External fixation by Ilizarov 3) antibiotics, hyperbaric oxygenation, vascular therapy 4) wound repair or skin plasty (no infection) 5) fracture repair by Ilizarov or intramedullary fixation.
Good luck!
Best wishes,
Date: Tue, 25 Feb 2003 07:22:39 -0500
From: Benedetti Gary E LtCol 74 MDOS/SGOSO
I agree with Dr. Starr: I&D, bridging external fixation, soft tissue control, with delayed internal fixation when the soft tissue is ready.
Gary E. Benedetti, LtCol, USAF, MC, FS
Orthopaedic Trauma Surgery
Date: Tue, 25 Feb 2003 09:11:10 -0500
From: James Carr
This is one of those injuries where you do what you do best. I would span the ankle with smooth tensioned wires in the calcaneus and proximal tibia. The fibula would be fixated initially only if exposed by the open wound- same applies to the tibia. Definitive fixation would be sub-q plating using the medial border of the tibia. Locking plates are a nice touch, but not a necessity as the tibia is not comminuted. The fibula needs plating as well- it may not be possible to get any screws distally due to comminution. Basically a long winded saying of I agree with the other posts.
James B. Carr, MD
Palmetto Health Orthopedics
Date: Fri, 28 Feb 2003 19:57:10 +0530
From: DR T I GEORGE
Friends,
Thank you all for the kind responses. Kindly find attached the post op picture. I did an Ilizarov ring fixation which extended to the calcaneum. There was multiple small areas of partial thickness skin necrosis anteriorly and laterally which required split thickness skin graft.
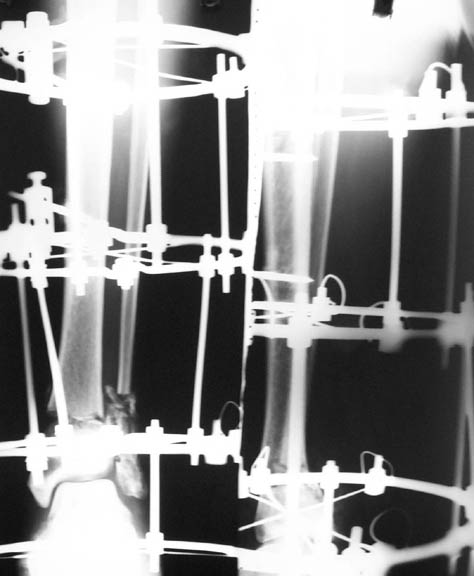 |
Request your further comments.
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.
Date: Fri, 28 Feb 2003 14:35:38 -0700
From: Terry Finlayson
Dr. George:
Ilizarov device is a good choice, but I'm concerned about the valgus angulation (> 15degrees ?).
Terry I. Finlayson, MD
Alpine Orthopaedic Specialists
Logan, UT
Date: Sat, 1 Mar 2003 12:59:50 +0530
From: Dr Mangal Parihar
george,
whenever possible, i avoid calcaneal rings for two reasons:
1. the wires tend to irritate/pain/discharge more than the other wires,
because they are put in under less tension
2. walking requires specially modified footwear with a raise
i would therefore, as a general rule, try my utmost to put in more wires in the distal fragment to gain a good hold + compression across the fracture site adds a lot to the stability of the frame. usually, in stable configuration of fractures, like your patient has, the calcaneal fixation then becomes redundant. you would need to compress this fracture further, judging from the xrays
mangal parihar
orthopedic surgeon, mumbai
Date: Sat, 1 Mar 2003 18:24:00 +0530
From: DR T I GEORGE
Dear Terry and Mangal,
Thanks for the input.
We noticed the valgus at the ankle and this was corrected at about three weeks from injury along with removal of calcaneal wires and skin grafting. I did not do a check-ray but used images in the II monitor. Subsequently we allowed partial weight bearing ambulation.
He was reviewed two days ago and we noticed a valgus position of the foot. This patient's relative is a senior Orthopaedic colleague of mine who said that patient's siblings have flatfeet and this was left out. On second thoughts we are wondering whether the talus slipped out laterally because the lateral malleolus is totally comminuted. We have asked the patient to report back to check radiologically if there is any subluxation or whether it is just flat foot which gives the impression of valgus foot.
Will keep you informed on follow up.
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.
Date: Sun, 2 Mar 2003 17:44:52 +0200
From: Dr Savvides
Dr. George:
Comments:
1. The reduction is in Valgus. Which you could correct on the Ilizarov and
2. The Lateral Malleolus is about 6mm superior to its normal position, which
I don't know how you could correct.
G. Savvides.
Date: Tue, 4 Mar 2003 02:25:31 +0500
From: Alexander Chelnokov
Hello DR,
DTIG> I did an Ilizarov ring fixation which extended to the calcaneum. There was multiple small areas of partial thickness skin
Why connecting rods are bent?
As Dr Finlayson commented the fragments are malaligned. The combination of wires and pins in the middle ring makes correction at least inconvenient though of course it is always possible to re-assembly the frame and include hinges.
It would be quite enough to have either a 6 mm half pin or a olive wire inserted in frontal plane just above the fracture. The pin or wire would help to move the distal part of the shaft laterally (and a bit back) to align the fracture.
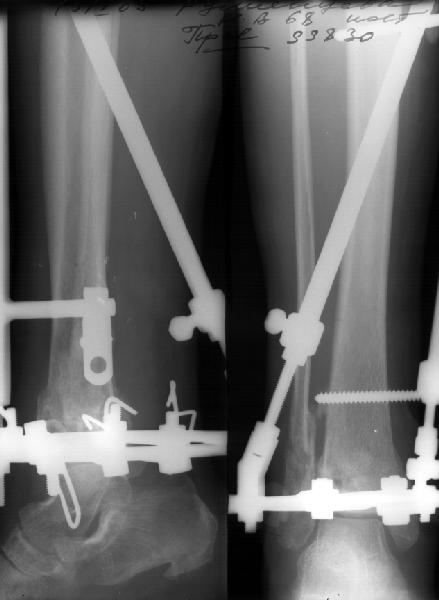
See an example of the suitable assembly. The injury is not so severe as in your case but the fracture pattern dictates a quite similar mounting. Since in your case the distal fragment is even larger than in the example there is no need to use foot extension as dr M. Parihar said. A foot support looks enough.
 |
 |
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Tue, 11 Mar 2003 23:24:51 +0530
From: DR T I GEORGE
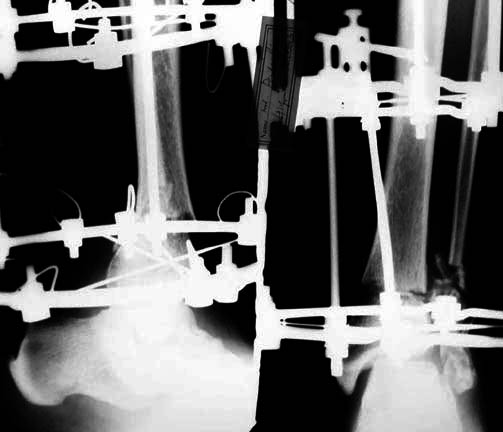
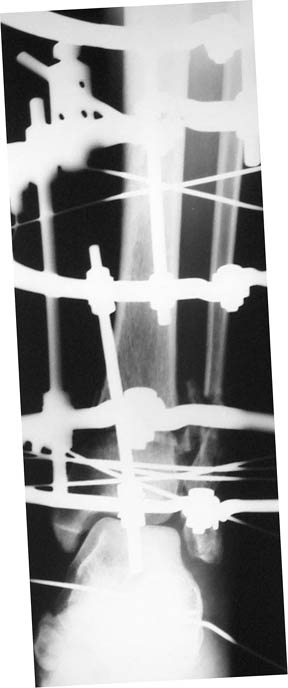
To give the follow up on this patient: A repeat X-ray showed the talus subluxating laterally. A dynamic inversion and eversion strain view pictures showed the lower tibio-fibular syndesmosis opening out. The frame was re-adjusted. Fracture site compressed and valgus corrected. A syndesmotic compression was achieved by adding a washer to the olive and pulling the comminuted lateral malleolus medially. another olive with washer given through talus lateromedially. The equinus that you may see has been corrected. Pictures attached. would welcome critical comments.
 |
 |
 |
 |
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.