{kind=link}



Date: Date: Sun, 22 Jul 2001 19:39:49 -0400
From: Amir Matityahu
Subject: Distal Clavicle Fx
A 44 year old male 220 lb, but lean, body builder was riding his bicycle at about 30 km/hr and fell off onto his left shoulder. He is right hand dominant. He has an abrasion 3 cm posterior to the acromioclavicular joint. His left shoulder is anterior and caudad relative to the right shoulder. He is neurovasculary intact.
Radiographs show a displaced lateral 1/3 clavicle fracture (Neer type II). There is an inferior butterfly fragment that the conoid and trapizoid ligament most likely attach to.
We have found that fixation of this fracture is difficult. Does anyone have any suggestions that may help this previously very strong patient that wants to return to his high level of activity?
Thank you for your suggestions in advance,
Amir Matityahu, MD
|
|
|
Date: Sun, 22 Jul 2001 23:21:24 -0400
From: Irving Strauchler
I would fix with 2 k-wires and figure 8 tension band as per AO technique.
I Strauchler MD
Date: Mon, 23 Jul 2001 07:28:52 -0700
From: John Ruth
I agree that fixation is difficult. Plate fixation is not optimum and frequently fails. I have had the best results with obtaining a healed and stable fracture using an open approach (vertical incision over the fracture) to first reduce and secure the medial fragment to the coracoid with a heavy nonabsorbable (#5 ticron) suture through drill holes in the medial clavicular fragment. This is followed by placement of Acromioclavicular screw. It is easiest to use a guide pin for a 4.5 cannulated screw placing it laterally through a separate stab incision between the table of the acromion and into the medullary canal of the clavicle. It is likely that the screw will exit the posterior-superior cortex of the medial fragment and this will improve fixation. I frequently remove the screw at about 3 months in the office.
Date: Mon, 23 Jul 2001 23:09:50 +0600
From: Alexander Chelnokov
Hello John,
JR> I agree that fixation is difficult. Plate fixation is not optimum and
Fixation is easy with external apparatus. Of course, it is a discomfort but mostly acceptable for 4-6 weeks needed for healing. The surgery is less than 30 minutes, a patient can leave for home at the same day.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
7, Bankovsky str. Ekaterinburg 620014 Russia
Date: Mon, 23 Jul 2001 15:55
From: Bill Burman
Some references which might be helpful for informed consent
From the OTA Archives - Kona, Bosse et al in 1987 reported on Type II Clavicle Fxs in a retrospective review of 20 patients with an avg 3.2 year followup published J Orthop Trauma 1990;4(2):115-20. There was a 45% complication rate with surgical treatment. Authors recommended conservative rx with a Kenny Howard brace and late excision of painful non-unions.
Here are 5/21 References from Medline using search terms "Neer Type II clavicle"
Conservative Rx:
Operative Rx
Date: Mon, 23 Jul 2001 22:16:06 -0400
From: Amir Matityahu
Dr Alexander Chelnokov,
RE: Fixation is easy with external apparatus
I have 2 questions regarding this approach. First, the lateral aspect of the clavicle is comminuted, and in my experience, soft bone. How do you construct the frame to pull up the shoulder and push down the clavicle. Second, do you have any clinical examples?
Regarding the literature, there are also reports of plate osteosynthesis. Does anyone have experience with this method? (Unfallchirurg 2000 Jul;103(7):538-44) As with difficult fractures, the literature is convincing in one thing: There is not an optimal way to fix this as of yet.
Amir Matityahu, M.D.
Date: Tue, 24 Jul 2001 17:32:45 +0600
From: Alexander Chelnokov
Hello Amir,
AM> I have 2 questions regarding this approach. First, the lateral aspect of the clavicle is comminuted, and in my experience, soft bone. How do you construct the frame to pull up the shoulder and push down the clavicle.
Biomechanics of the injury requires the same ex-fix approach as for ACJ dislocation. So a lateral reference wire is placed into the acromion.
 |
 |
 |
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
7, Bankovsky str. Ekaterinburg 620014 Russia
Date: Tues, 24 Jul 2001 08:39
From: Bill Burman
Alex
While your ex fix rx of a Type 3 AC injury looks impressive, what about the risk of the placement of medial clavicular pins to major intrathoracic anatomy?
Medial clavicular pins used for SC joint fixation have a high complication rate. According to the 1996 AAOS Orthopaedic Knowledge Update for Trauma:
"Because of the widely reported complications of Kirschner wire fixations of the sternoclavicular joint, such misadventures are to be condemned. One author, in his report of intrathoracic dislocation of Kirschner wires after fixation of these injuries, suggested that this problem "requires treatment by a surgeon with good experience in thoracic surgery."
Date: Tue, 24 Jul 2001 22:03:55 +0600
From: Alexander Chelnokov
Hello Bill,
BB> what about the risk of the placement of medial clavicular pins to major intrathoracic anatomy
The wires are inserted downwards and in slightly anterior direction, to be parallel to anterior chest wall. So no interference can happen with any intrathoracic structure.
BB> Medial clavicular pins used for SC joint fixation have a high complication
It is a _completely_ different story. The wires/pins are inserted not that way and place i meant, and not secured to an external fixator. BTW i am not aware of a reliable ex-fix method for SC dislocations, opposite to ACJ.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
7, Bankovsky str. Ekaterinburg 620014 Russia
Date: Tue, 24 Jul 2001 21:43:45 -0400
From: Amir Matityahu
Thank you all for a very interesting discussion.
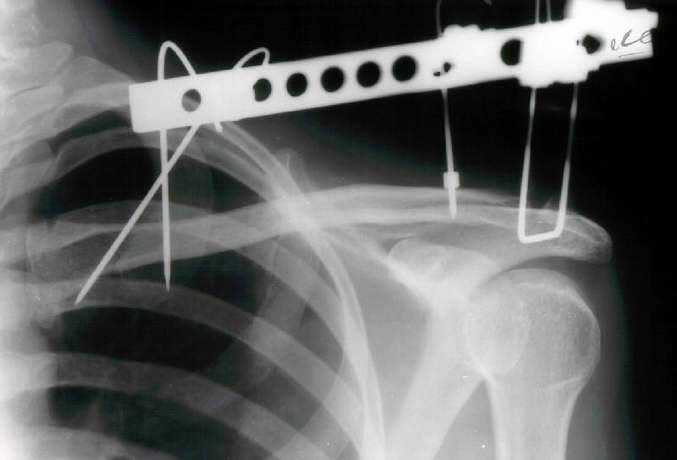
Since we have no experience with external fixation of the clavicle, we did not use this method. However, it is very interesting to see. We elected to use a T plate with a screw into the coracoid as shown in the X-ray below.
 |
Any comments would be appreciated.
Thank you,
Amir Matityahu MD
Date: Wed, 25 Jul 2001 09:47:14 +0600
From: Alexander Chelnokov
Hello Amir,
AM>We elected to use a T plate with a screw. Any comments would be appreciated.
Looks pretty fine!
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
7, Bankovsky str. Ekaterinburg 620014 Russia
Date: Sat, 28 Jul 2001 07:30:51 +0300
From: Monhamed Abdel-All
It is a very interesting fixation but i think that the coracoid screw insertion is a little bit difficult . I have some experience in doing coraco-clavicular screw fixation and I found marked difficulty to introduce the screw.