
Date: Mon, 13 May 2002 23:55:56 +0600
Subject: Comminuted femur fx
Hello All,
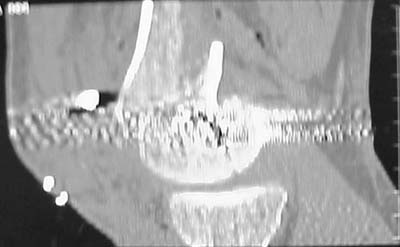
A male 31 y.o. addmitted to our unit today with the subject (see attachment). Injured in a car accident 1 month ago, since that he has been at bed traction. Other fractures are minor - undisplaced pubic rami and distal ulna.
|
What is your opinion about optimal program here? Is closed nailing a good option here? Articular part of condyles looks fine, but the lateral one seems to be too small and comminuted. Or external fixation as definitive method? Or open the fracture at least distally, fix condyles then nail?
THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 13 May 2002 13:52:44 -0400
From: Andrea Salvi
Dear colleague,
Of course the only radiograms both the view of the femur (AP and LL) are not enough in order to assess the condyles. So I think a TAC of the knee could be useful.
If you're going to use a nail, it could be blocked proximally and distally, because of the spiroid rime of the fracture. But, in my opinion, the real problem is the distal fracture and so I suggest the use of a long plate, to include the condyles with 5 metal cerclage rings (Zuggurtung) for re-inforcement along the plate or a external fixator. Because of the risk of stiffness (keeping the knee moving in a passive motion, using, for example, a Kinetec device).
Best Regards
Dr Andrea Salvi
Spedali Civili
BRESCIA - ITALY
2 Divisione Ortopedia-Traumatologia
Date: Mon, 13 May 2002 13:18:41 -0600
From: Thomas A. DeCoster
consider retrograde IM nail with distal fragment screw fixation as needed
td
Date: Mon, 13 May 2002 17:13:21 -0400
From: William Obremsky
A CT and knee xrays would help identify lateral condyle comminution and/or a "hoffa fragment" of the posterior condyle. I am concerned that the lateral cortex is not sufficient to give purchase for a retrograde IMN. blocking screws could improve this as a possibility.
A long blade or LISS if avaible would be my secondary choices.
Good luck.
Any chance you can get these cases transferred earlier when it would be less difficult?
Bill Obremskey
Date: Tue, 14 May 2002 08:00:50 +0100
From: Peter Hamilton
Distal articular reduction /fixation with retrograde IM nail or long LISS plate.
PH
Date: Tue, 14 May 2002 13:03:51 +0600
From: Alexander Chelnokov
Hello William,
WO> cortex is not sufficient to give purchase for a retrograde IMN. blocking screws could improve this as a possibility.
How the screws should be placed?
WO> A long blade or LISS if avaible would be my secondary choices.
Lateral condyle looks too small for the blade, and the plate too short.
WO> Any chance you can get these cases transferred earlier when it would be less difficult?
Unpredictable.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Tue, 14 May 2002 08:07:21 -0400
From: William Obremsky
How the screws should be placed?
Use 6.5 mm cannulated screws if you have and place one anterior to where IMN will go if anterior cortex if insufficient and AP screws on either side of the IMN out of the trochlea to provide some additional varus/valgus stability. I worry about the leg going into valgus w/ the lack of lateral cortex.
See attached case that was done several years ago before LISS. He had comminuted trochlea and anterior blocking screws were used to prevent anterior IMN cut-out.
 |
 |
 |
 |
 |
 |
Good luck.
Bill Obremskey
Date: Wed, 15 May 2002 09:37:03 +0600
From: Alexander Chelnokov
Hello William,
WO> Use 6.5 mm cannulated screws if you have and palce one anterior to where IMN will go if anterio cortex if insufficient
I plan to place wires before nail insertion, and 6,5 mm screws after nail is in place.
WO> and AP screws on either side of the IMN out of the trochlea to provide some additional varus/valgus stability.
Will look into it.
WO> I worry about the leg going into valgus w/ the lack of lateral cortex.
It is under control if external fixator is used.
WO> See attached case that was done several years ago
THX for the case. Very impressive. Was so fine reduction made by closed way?
WO> before LISS.
Do you suppose LISS superior to closed IM nailing for such cases?
WO> Good luck.
THX. The case is scheduled for today.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Thu, 16 May 2002 17:22:29 +0600
From: Alexander Chelnokov
Hello All,
Yesterday antegrade closed nailing was performed (UFN 10 mm). Two cancellows screws added to fix the lateral condyle. The surgery was not too easy, and extension of condylar part i failed to reduce completely. The shaft looks even more ugly. The patient left for a couple of days in 90/90 position. Comments/opinions/advices are welcome.
 |
THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Thu, 16 May 2002 07:41:10 -0400
From: William Obremsky
Since it was done closed the shaft will heal or at worst need an exchange IMN.
Nice job.
Bill O
Date: Thu, 16 May 2002 06:18:32 -0700 (PDT)
From: Zsolt Balogh
Alex,
Congratulations! Tough case. I think you achieved the best achievable result which possible with this method for this complex injury.
What does "a couple of days" mean?
Best Regards,
Zsolt Balogh
Date: Thu, 16 May 2002 23:43:54 +0600
From: Alexander Chelnokov
Hello Zsolt,
ZB> Congratulations! Tough case. I think you achieved the ZB> best achievable result which possible with this method
I'd like to learn what benefits retrograde nailing offers for such cases. How reduction is performed in case of retrograde nail? Here i used a distractor with crossing wires which wouldn't allow to insert nail from the knee.
ZB> What does "a couple of days" mean?
I mean that the patient was positioned with hip and knee flexed to 90 degrees for two first postoperative days.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 20 May 2002 13:53:27 -0600
From: Thomas A. DeCoster
Regarding your case
IM nails are very forgiving but there are limits. I've seen cases with this postop appearance heal nicely.
The advantages of retrograde nail in this situation are: easier insertion, easier reduction and better distal fixation.
See AAOS website OKO (Orthopaedic Knowledge Online) for discussion of retrograde and antegrade femoral nailing with audio pros and cons from Drs. Swiontowski and Watson, video demonstrating techniques, case examples with 10 year followup etc. http://www.aaos.org then click on oko
OKO is also available directly to AAOS members and others who subscribe. Other topics are also presented and many other topics are coming online each year.
Tom DeCoster