Date: Thu, 7 Mar 2002 00:57:26 +0500
Subject: Distal Femoral Fracture
Hello All,
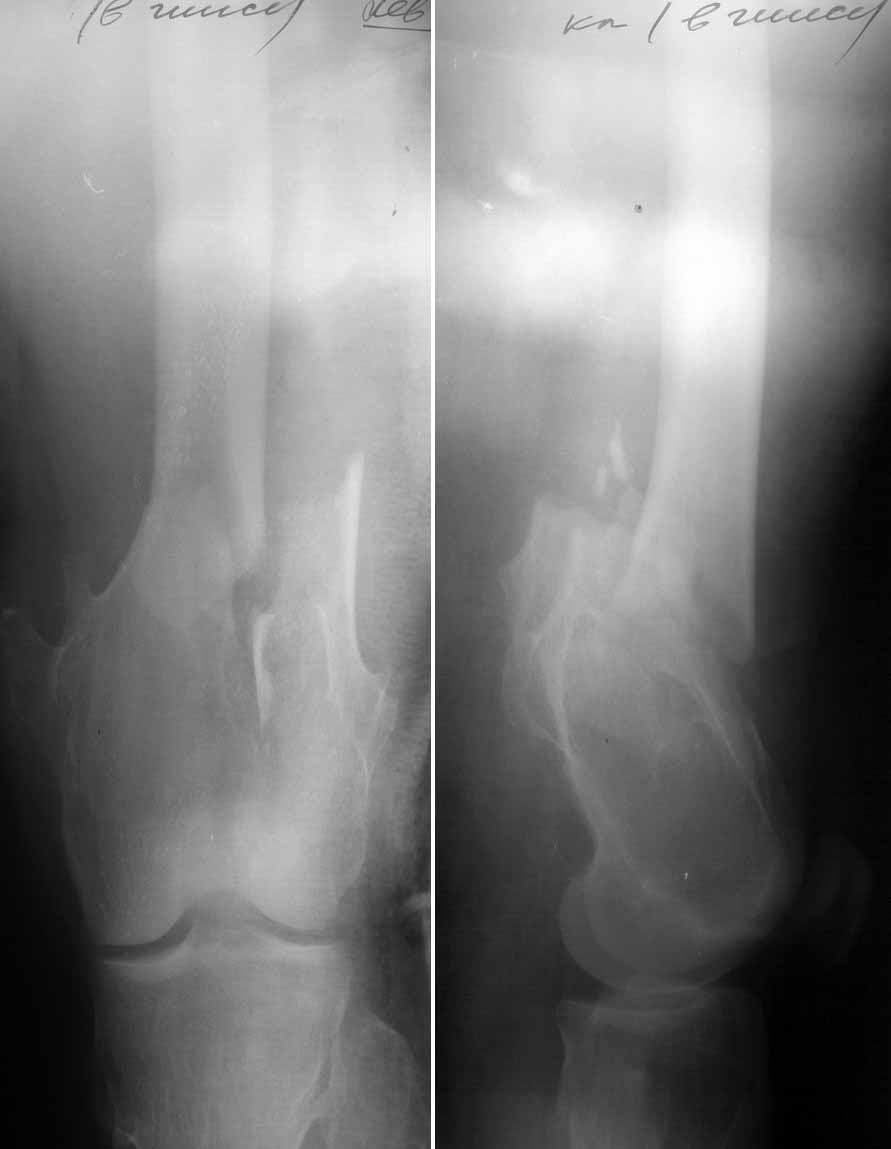
A woman 39 y.o. admitted to our unit 2 weeks after a car accident (was a passenger). She sustained T-shape distal femoral fracture, condyles haven't been displaced (yet :-).
|
She also has fractured III-IV right metacarpal bones. All x-rays reveal some skeletal disorder with multiple bone deformations and exostoses which didn't troubled her before maybe because her obesity.
What would be optimal treatment plan?
Anyway I plan to start with attempt of closed IM nailing which can be problematic in our settings if medullary canal is to narrow because we still don't have flexible reamers. She lives far from our city so i don't want to leave her with external fixator. DCS, condylar or blade plate?
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 06 Mar 2002 16:03:51 -0500
From: James Carr
What do you think that is in the femur? I guess an enchondroma, but am a bit rusty on that stuff. I am one of those guys who would nail it retrograde thru a medial patellar approach. Obese folk are difficult regardless, but I think they do better with IM fixation.
Jim Carr
Date: Wed, 06 Mar 2002 14:41:12 -0600
From: Adam Starr
Howdy Alex.
There are surgeons who treat these sort of injuries with a locked retrograde IM nail, but I prefer an open reduction and fixation with a plate. I'd use a DCS or a blade plate.
They're fun cases in young patients with good bone. Less fun in elderly patients with poor bone. Obese patients are no fun no matter how old they are.
Good luck,
Adam Starr
Dallas
Date: Wed, 06 Mar 2002 16:33:56 -0500
From: William Obremsky
It looks like the split goes into the intercondylar notch. Screw fixation of the condyles and a retrograde IMN would be a good option. She seems to have a big canal to go w/ her big body and you could get a large IMN w/o reaming since that is a problem.
Bill Obremskey
Date: Thu, 7 Mar 2002 18:58:51 +0100
From: Josep M. Munoz Vives
Due to poor quality of the films I can't assure it but there may be a large third fragment in the external metaphysis. If it is the case it may compromise locking screws purchase in retrograde or antegrade nailing, at least the most proximal one.
Probably it is not yet available to you, but I think that LISS (percutaneous) plating could be another option with better purchase in the distal fragment.
Dr. Josep M. Munoz-Vives
Orthopedic Surgery Dept.
Hospital Dr. Josep Trueta
Girona - Catalunya
Spain
Date: Fri, 08 Mar 2002 14:07:58 -0700
From: Thomas A. DeCoster
Dr. Chelnokov,
Retrograde nail is a good option and flexible reamers not absolutely required in this kind of patient. Lateral plate can also give good results but requires a lot more dissection (especially with obesity) and the bone purchase is not very reliable with osteopenia and surface irregularities (her bone disease) is more problematic than with nail. Distal screws outside the nail (anterior and perhaps posterior) are helpful and you can get distal fixation through the nail even though this fracture is fairly distal.
Best regards
TD
Date: Sat, 9 Mar 2002 13:06:54 +0500
From: Alexander Chelnokov
Hello James,
JC> What do you think that is in the femur? I guess an enchondroma
I am also wondering what skeletal disorder she presents. She also has metacarpals fracture and i made its film along with forearm and elbow which are also impressive, i attached one view.
 |
Maybe somebody can hint what exactly it is.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Sat, 9 Mar 2002 06:59:56 -0500
From: Tom Kaplan
Looks like it might be a case of a distal ulnar osteochondroma in the setting of multiple hereditary exostosis, with a secondary Madelung-type deformity of the distal radius.
Tom Kaplan
Date: Sat, 9 Mar 2002 09:45
From: Bill Burman
>Looks like it might be a case of a distal ulnar osteochondroma in the setting of multiple hereditary exostosis, with a secondary Madelung-type deformity of the distal radius
This case appears to be a multiple hereditary exostosis (MHE)
However, strictly speaking, I believe the classic Madelung's deformity (which can be caused by MHE)
see: http://www.rad.washington.edu/maintf/cases/unk53/answers.html
refers to a relative radial shortening rather than the relative ulnar shortening seen in this patient's forearm.
Bill Burman, MD
HWB Foundation
Date: Mon, 11 Mar 2002 23:35:05 +0500
From: Alexander Chelnokov
Hello All,
THX to all for suggestions. We don't have implants for retrograde nailing through the knee. BTW - can UFN be used for retrograde nailing? Franlky speaking i don't understand why it must be better than antegrade. Fortunately the attempt of antegrade closed static IM nailing was successful. I used UFN 9 mm, and minimal reaming was necessary to fit. I prepared improvized hand reamer from titanium rod which was flexible enough to reach the isthmus located just above the fracture. The bone was quite porotic. Condyles were additionally fixed by a cancellows screw. I've never used distal locking screws 85 mm long before.
 |
Comments are welcome. THX.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 11 Mar 2002 11:59:31 -0800
From: Carlo Bellabarba
Hi Alex,
You can use many of the standard nails through the retrograde approach if you want, particularly if the fracture isn't that distal. last i checked, this was a much cheaper way to nail femurs retrograde, even in this part of the world, although that may have changed of late. the real advantage of nails designed specifically for retrograde use are the more distal interlocking screw holes and the anterior-to-posterior proximal locking screw orientation (especially easier in the obese).
Nails that don't do so well when turned around and placed retrograde are those with only oblique "proximal" interlocking screws (ie distal when retrograde), and those like the synthes universal nail where the "proximal" end of the nail flares considerably.
Carlo Bellabarba
Seattle
Date: Tue, 12 Mar 2002 07:08:01 -0500
From: James Carr
I once looked at it, and many antegrade nails actually have more distal screws than their retrograde counterparts. The other advantages are as stated.
Date: Tue, 12 Mar 2002 08:48:14 +0530
From: DR T I GEORGE
I have seen a surgeon use tibial nail as retrograde on femur. He was not keen on proximal interlocking since the proximal end of nail will be thru the isthmus of femur. What is the list members experience/opinion on leaving the proximal end unlocked?
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.
Date: Tue, 12 Mar 2002 07:09:27 -0500
From: James Carr
The concerns are the same as any femoral nailing: rotation and shortening in unstable fx patterns. Probably works fine in stable patterns in most cases.
Date: Tue, 12 Mar 2002 21:15:19 +0200
From: Yalim Ates
We sometimes use a femoral nail retrograde on the femur. Have not locked the proximal part (through the distal end of the nail) and have had no problems yet (did about 10) years.
Yalim Ates MD
SSK Ankara Teaching Hospital